

Defining Clinical Subgroups in Relapsing Polychondritis: A Prospective Observational Cohort Study
- PMID: 32249511
- PMCID: PMC8672710
- DOI: 10.1002/art.41270
Defining Clinical Subgroups in Relapsing Polychondritis: A Prospective Observational Cohort Study
Abstract
Objective: Relapsing polychondritis (RP) is a systemic disease. Failure to recognize RP can lead to diagnostic delay and further complications, including death. This study was undertaken to identify clinical patterns in a prospective cohort of patients with RP.
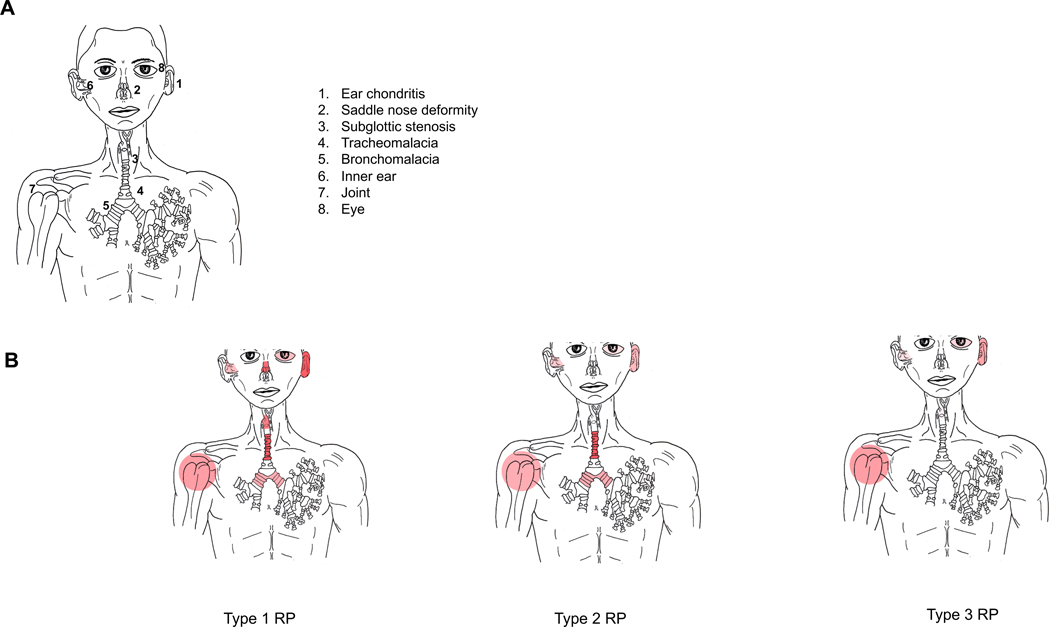
Methods: Patient subgroups were identified using latent class analysis based on 8 clinical variables: saddle-nose deformity, subglottic stenosis, tracheomalacia, bronchomalacia, ear chondritis, tenosynovitis/synovitis, inflammatory eye disease, and audiovestibular disease. Model selection was based on Akaike's information criterion.
Results: Seventy-three patients were included in this study. Patients were classified into 1 of 3 subgroups: type 1 RP (14%), type 2 RP (29%), and type 3 RP (58%). Type 1 RP was characterized by ear chondritis (100%), tracheomalacia (100%), saddle-nose deformity (90%), and subglottic stenosis (80%). These patients had the shortest median time to diagnosis (1 year), highest disease activity, and greatest frequency of admission to the intensive care unit and tracheostomy. Type 2 RP was characterized by tracheomalacia (100%) and bronchomalacia (52%), but no saddle-nose deformity or subglottic stenosis. These patients had the longest median time to diagnosis (10 years) and highest percentage of work disability. Type 3 RP was characterized by tenosynovitis/synovitis (60%) and ear chondritis (55%). There were no significant differences in sex, race, or treatment strategies between the 3 subgroups.
Conclusion: Our findings indicate that there are 3 subgroups of patients with RP, with differences in time to diagnosis, clinical and radiologic characteristics, and disease-related complications. Recognizing a broader spectrum of clinical patterns in RP, beyond cartilaginous involvement of the ear and upper airway, may facilitate more timely diagnosis.
© 2020 American College of Rheumatology. This article has been contributed to by US Government employees and their work is in the public domain in the USA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Reply.Arthritis Rheumatol. 2020 Dec;72(12):2167-2168. doi: 10.1002/art.41438. Epub 2020 Oct 7. Arthritis Rheumatol. 2020. PMID: 32686916 No abstract available.
-
Early Recognition of Relapsing Polychondritis: Comment on the Article by Ferrada et al.Arthritis Rheumatol. 2020 Dec;72(12):2166-2167. doi: 10.1002/art.41439. Epub 2020 Oct 11. Arthritis Rheumatol. 2020. PMID: 32686919 No abstract available.
References
-
- Sane DC, Vidaillet HJ Jr, Burton CS Iii: Saddle nose, red ears, and fatal airway collapse.Chest 1987, 91(2):268–270. - PubMed
-
- Dion J, Costedoat-Chalumeau N, Sene D, Cohen-Bittan J, Leroux G, Francés C, Piette JC. Description of 142 cases of relapsing polychondritis followed in a single center since 2000. Arthritis and rheumatism 2013, 65:S868.
-
- Dion J, Costedoat-Chalumeau N, Sene D, Cohen-Bittan J, Leroux G, Dion C, et al. Relapsing Polychondritis Can Be Characterized by Three Different Clinical Phenotypes: Analysis of a Recent Series of 142 Patients. Arthritis Rheumatol 2016, 68(12):2992–3001. - PubMed
-
- Michet CJ Jr, McKenna CH, Luthra HS, O’Fallon WM. Relapsing polychondritis: Survival and predictive role of early disease manifestations. Annals of internal medicine 1986, 104(1):74–78. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
