

Sex-specific sagittal and frontal plane gait mechanics in persons post-hip arthroscopy for femoroacetabular impingement syndrome
- PMID: 32249962
- PMCID: PMC7541416
- DOI: 10.1002/jor.24680
Sex-specific sagittal and frontal plane gait mechanics in persons post-hip arthroscopy for femoroacetabular impingement syndrome
Abstract
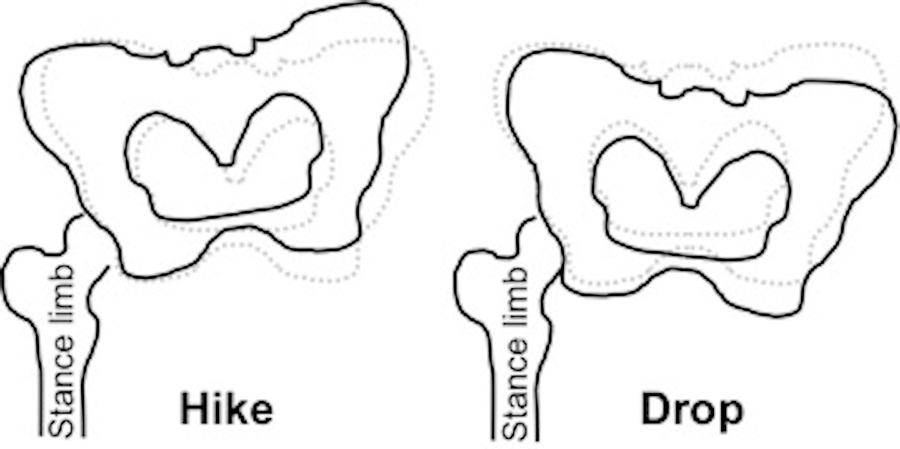
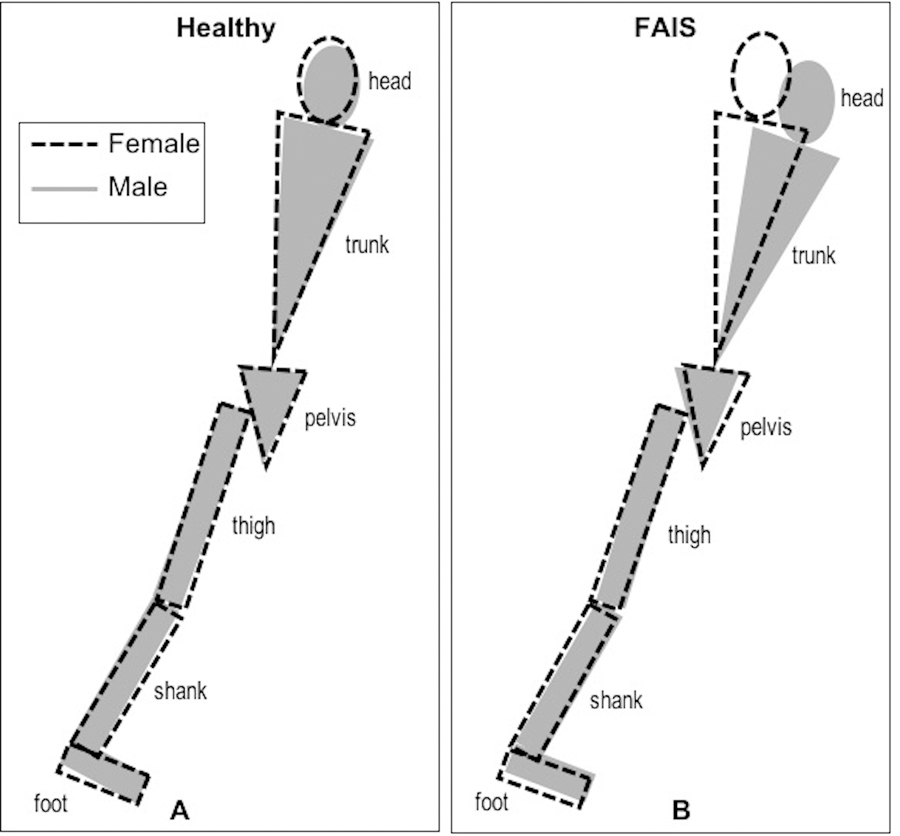
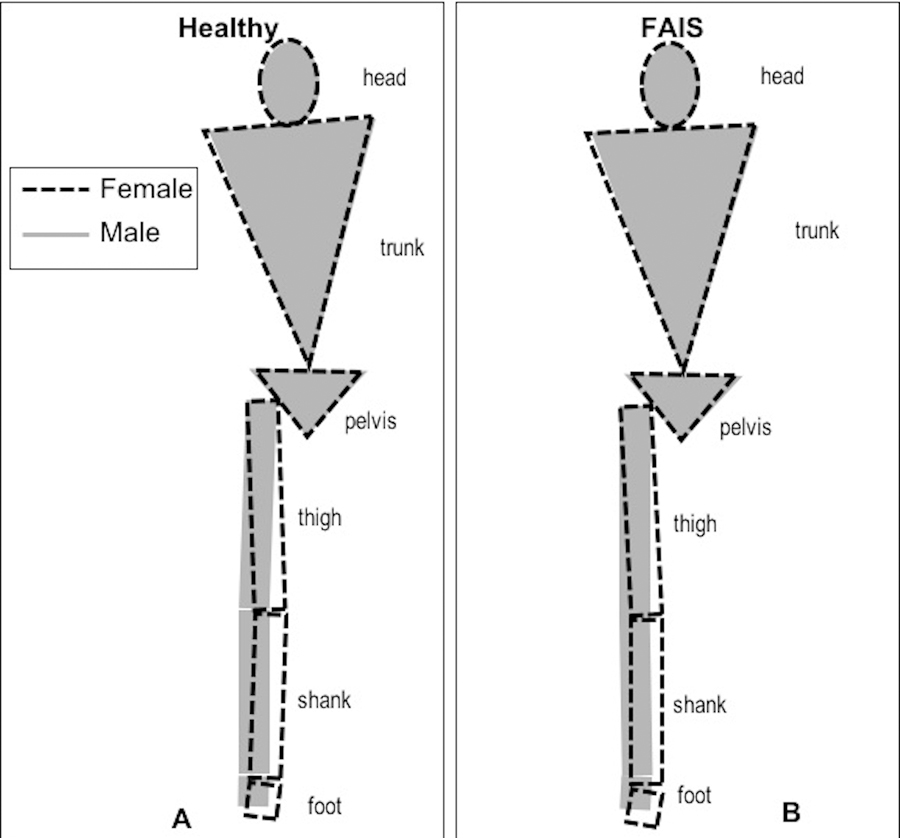
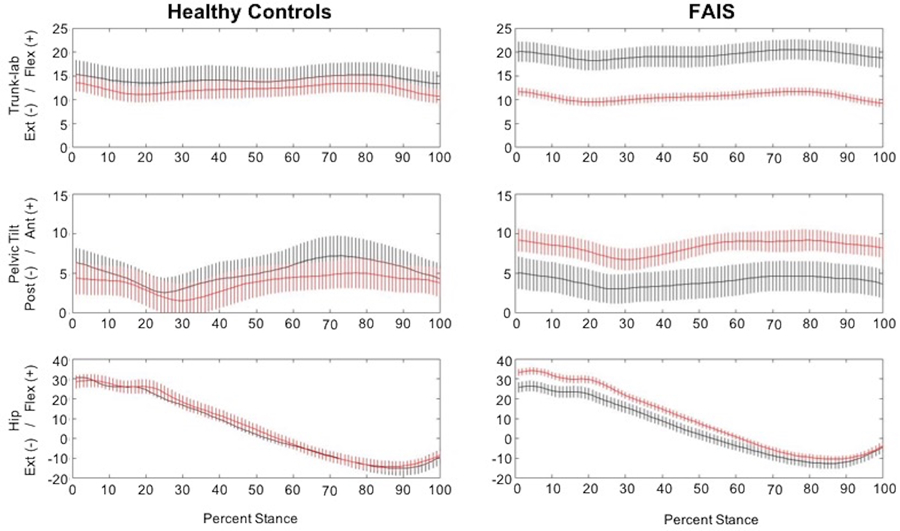
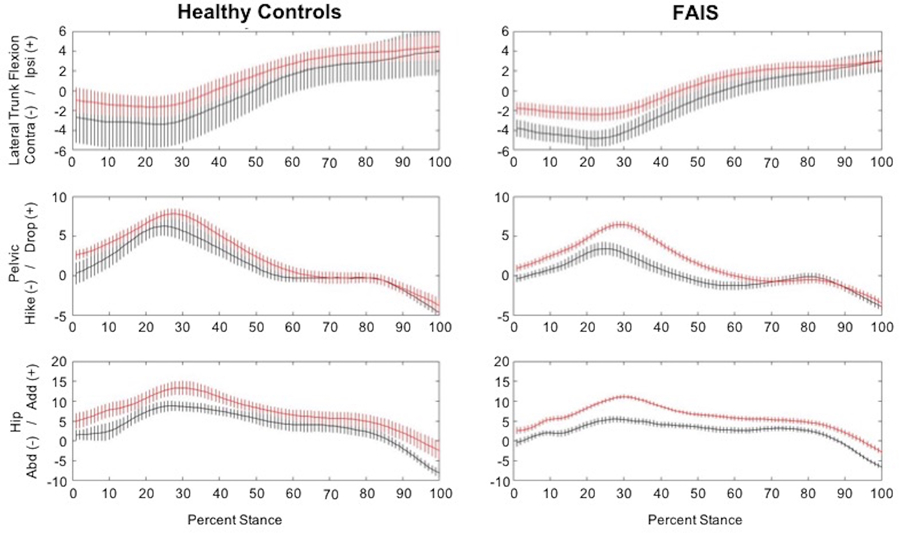
Postoperative gait mechanics in persons with femoroacetabular impingement syndrome (FAIS) remain understudied as a treatment outcome despite observed, yet inconclusive, preoperative gait abnormalities. Females with FAIS demonstrate worse preoperative patient-reported hip function and altered hip mechanics when compared with males; it is unknown whether these sex differences persist postarthroscopy. The purpose of this study was to compare sex-specific gait kinematics between persons at least 1 year postarthroscopy for FAIS and healthy comparisons. General linear models with estimating equations were used to evaluate the effect of (a) limb and sex within each group, and (b) limb and group within each sex for peak sagittal and frontal plane trunk, pelvis, and hip kinematics during stance phase of gait. Analyses were covaried by gait speed. Seventeen females and eight males an average 2.5 years postarthroscopy (1.1-7.2 year) for FAIS were compared with healthy females (n = 7) and males (n = 5). Females in the FAIS group presented with an average of 4.6° more anterior pelvic tilt, and 4.8° less hip extension compared with healthy females (P ≤ .03) and 8.6° less trunk flexion, 4.8° more anterior pelvic tilt, 3.1° more pelvic drop, and 7.5° more hip flexion than males with FAIS (P ≤ .03). Males in the FAIS group presented with 2.9° less pelvic drop, and 3.2° less hip adduction than healthy males. Preoperative gait mechanics were not collected and thus changes in mechanics could not be evaluated. This study is significant to clinicians who treat patients postarthroscopy to consider sex-specific gait impairments.
Keywords: FAI; gender; kinematics; walking.
© 2020 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
Figures
References
-
- Griffin D, Dickenson E, O’Donnell J, et al. The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sport Med 2016;50(19):1169–1176. - PubMed
-
- Frank JM, Harris JD, Erickson BJ, et al. Prevalence of femoroacetabular impingement imaging findings in asymptomatic volunteers: A systematic review. Arthroscopy 2015;31(6):1199–1204. - PubMed
-
- Heerey JJ, Kemp JL, Mosler AB, et al. What is the prevalence of imaging-defined intra-articular hip pathologies in people with and without pain? A systematic review and meta-analysis. Br J Sport Med 2018;52(9):581–593. - PubMed
-
- Levy DM, Kuhns BD, Chahal J, et al. Hip arthroscopy outcomes with respect to patient acceptable symptomatic state and minimal clinically important difference. Arthroscopy 2016;32(9):1877–1886. - PubMed
-
- King MG, Lawrenson PR, Semciw AI, Middleton KJ, Crossley KM. Lower limb biomechanics in femoroacetabular impingement syndrome: A systematic review and meta-analysis. Br J Sport Med 2018;52(9):566–580. - PubMed
Publication types
MeSH terms
Grants and funding
- K23 AR063235/AR/NIAMS NIH HHS/United States
- F30HD094520/National Center for Medical Rehabilitation Research/International
- TL1 TR002735/TR/NCATS NIH HHS/United States
- KL2TR002734/TR/NCATS NIH HHS/United States
- R01 AR070486/AR/NIAMS NIH HHS/United States
- KL2 TR002734/TR/NCATS NIH HHS/United States
- F30 HD094520/HD/NICHD NIH HHS/United States
- TL1TR002735/TR/NCATS NIH HHS/United States
- UL1 TR000090/TR/NCATS NIH HHS/United States
- 8UL1TR000090-05/TR/NCATS NIH HHS/United States
- KL2TR001068/TR/NCATS NIH HHS/United States
- UL1TR002733/TR/NCATS NIH HHS/United States
- UL1 TR002733/TR/NCATS NIH HHS/United States
- KL2 TR001068/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
