

Implementation of a Prehospital Stroke Triage System Using Symptom Severity and Teleconsultation in the Stockholm Stroke Triage Study
- PMID: 32250423
- PMCID: PMC7136864
- DOI: 10.1001/jamaneurol.2020.0319
Implementation of a Prehospital Stroke Triage System Using Symptom Severity and Teleconsultation in the Stockholm Stroke Triage Study
Abstract
Importance: To our knowledge, it is unknown whether a prehospital stroke triage system combining symptom severity and teleconsultation could accurately select patients for primary stroke center bypass and hasten delivery of endovascular thrombectomy (EVT) without delaying intravenous thrombolysis (IVT).
Objective: To evaluate the predictive performance of the newly implemented Stockholm Stroke Triage System (SSTS) for large-artery occlusion (LAO) stroke and EVT initiation. Secondary objectives included evaluating whether the Stockholm Stroke Triage System shortened onset-to-puncture time for EVT and onset-to-needle time (ONT) for IVT.
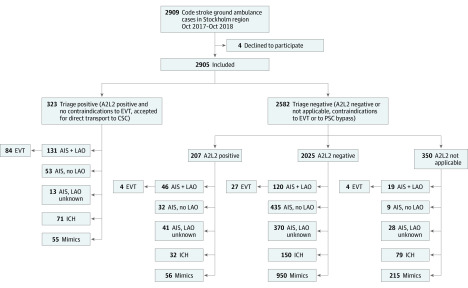
Design, setting, and participants: This population-based prospective cohort study conducted from October 2017 to October 2018 across the Stockholm region (Sweden) included patients transported by first-priority ("code stroke") ambulance to the hospital for acute stroke suspected by an ambulance nurse and historical controls (October 2016-October 2017). Exclusion criteria were in-hospital stroke and helicopter or private transport. Of 2909 eligible patients, 4 (0.14%) declined participation.
Exposures: Patients were assessed by ambulance nurses with positive the face-arm-speech-time test or other stroke suspicion and were evaluated for moderate-to-severe hemiparesis (≥2 National Institutes of Health stroke scale points each on the ipsilateral arm and leg [A2L2 test]). If present, the comprehensive stroke center (CSC) stroke physician was teleconsulted by phone for confirmation of stroke suspicion, assessment of EVT eligibility, and direction to CSC or the nearest primary stroke center. If absent, the nearest hospital was prenotified.
Main outcomes and measures: Primary outcome: LAO stroke. Secondary outcomes: EVT initiation, onset-to-puncture time, and ONT. Predictive performance measures included sensitivity, specificity, positive and negative predictive values, the overall accuracy for LAO stroke, and EVT initiation.
Results: We recorded 2905 patients with code-stroke transports (1420 women [49%]), and of these, 323 (11%) had A2L2+ teleconsultation positive results and were triaged for direct transport to CSC (median age, 73 years [interquartile range (IQR), 64-82 years]; 55 women [48%]). Accuracy for LAO stroke was 87% (positive predictive value, 41%; negative predictive value, 93%) and 91% for EVT initiation (positive predictive value, 26%; negative predictive value, 99%). Endovascular thrombectomy was performed for 84 of 323 patients (26%) with triage-positive results and 35 of 2582 patients (1.4%) with triage-negative results. In EVT cases with a known onset time (77 [3%]), the median OPT was 137 minutes (IQR, 118-180; previous year, 206 minutes [IQR, 160-280]; n = 75) (P < .001). The regional median ONT (337 [12%]) was unchanged at 115 minutes (IQR, 83-164; previous year, 115 minutes [IQR, 85-161]; n = 360) (P = .79). The median CSC IVT door-to-needle time was 13 minutes (IQR, 10-18; 116 [4%]) (previous year, 31 minutes [IQR, 19-38]; n = 45) (P < .001).
Conclusions and relevance: The Stockholm Stroke Triage System, which combines symptom severity and teleconsultation, results in markedly faster EVT delivery without delaying IVT.
Conflict of interest statement
Figures

Comment in
-
Triage Based on Preclinical Scores-Low-Cost Strategy for Accelerating Time to Thrombectomy.JAMA Neurol. 2020 Jun 1;77(6):681-682. doi: 10.1001/jamaneurol.2020.0113. JAMA Neurol. 2020. PMID: 32250425 No abstract available.
References
-
- Emberson J, Lees KR, Lyden P, et al. ; Stroke Thrombolysis Trialists’ Collaborative Group . Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384(9958):1929-1935. doi:10.1016/S0140-6736(14)60584-5 - DOI - PMC - PubMed
