

Defining Undertreatment and Overtreatment in Older Adults With Cancer: A Scoping Literature Review
- PMID: 32250717
- PMCID: PMC7392742
- DOI: 10.1200/JCO.19.02809
Defining Undertreatment and Overtreatment in Older Adults With Cancer: A Scoping Literature Review
Abstract
Purpose: The terms undertreatment and overtreatment are often used to describe inappropriate management of older adults with cancer. We conducted a comprehensive scoping review of the literature to clarify the meanings behind the use of the terms.
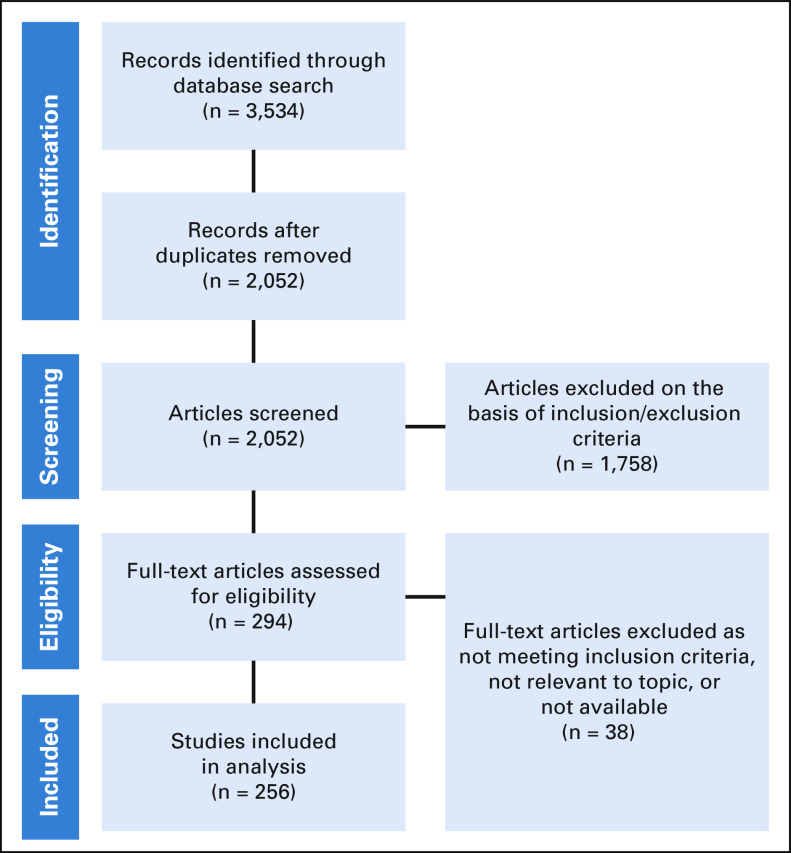
Methods: We searched PubMed (National Center for Biotechnology Information), Embase (Elsevier), and CINAHL (EBSCO) for titles and abstracts that included the terms undertreatment or overtreatment with regard to older adults with cancer. We included all types of articles, cancer types, and treatments. Definitions of undertreatment and overtreatment were extracted, and categories underlying these definitions were derived through qualitative analysis. Within a random subset of articles, C.D. and K.P.L. independently performed this analysis to determine final categories and then independently assigned these categories to assess inter-rater reliability.
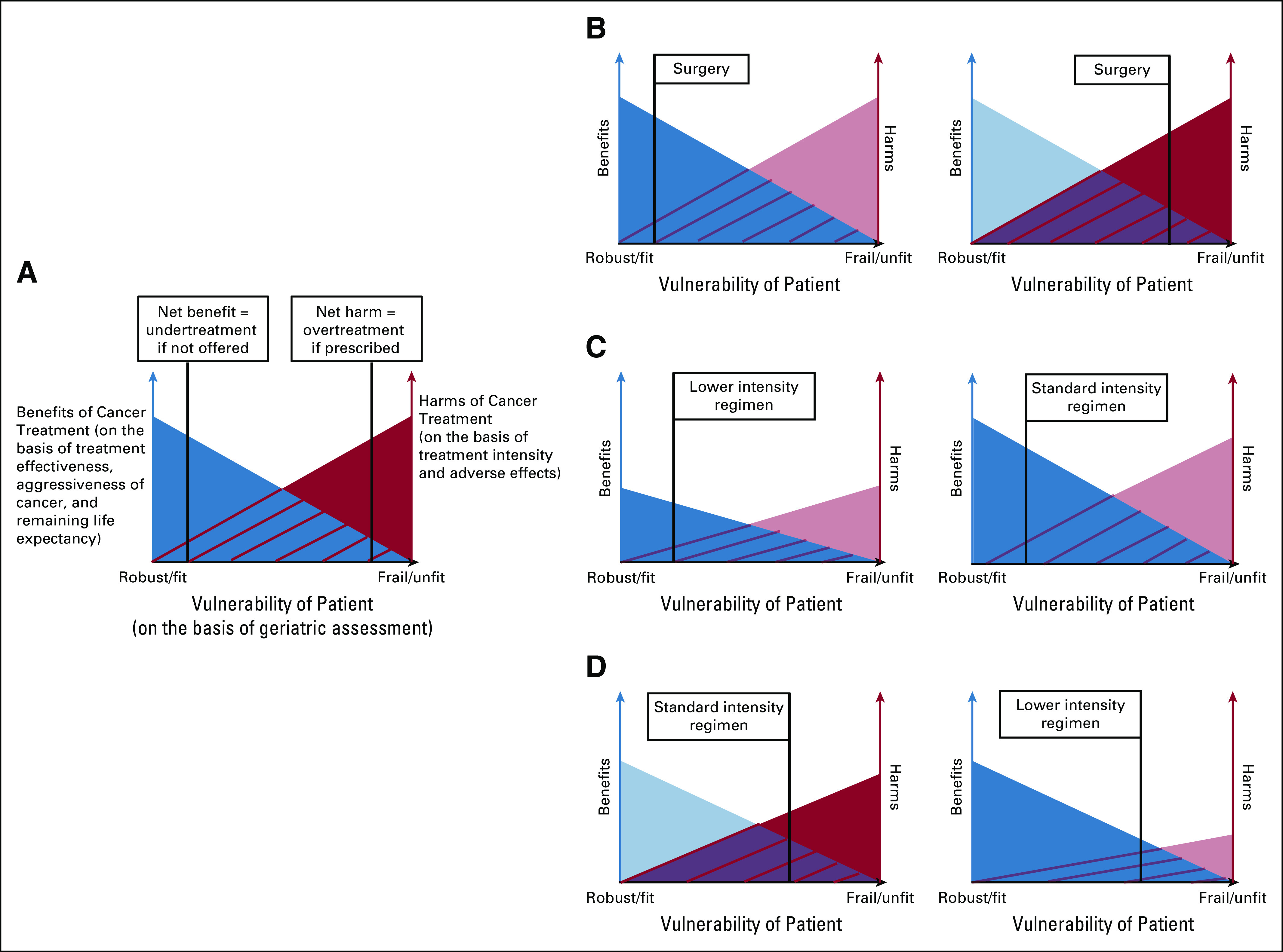
Results: Articles using the terms undertreatment (n = 236), overtreatment (n = 71), or both (n = 51) met criteria for inclusion in our review (n = 256). Only 14 articles (5.5%) explicitly provided formal definitions; for the remaining, we inferred the implicit definitions from the terms' surrounding context. There was substantial agreement (κ = 0.81) between C.D. and K.P.L. in independently assigning categories of definitions within a random subset of 50 articles. Undertreatment most commonly implied less than recommended therapy (148; 62.7%) or less than recommended therapy associated with worse outcomes (88; 37.3%). Overtreatment most commonly implied intensive treatment of an older adult in whom the harms of treatment outweigh the benefits (38; 53.5%) or intensive treatment of a cancer not expected to affect an older adult in his/her remaining lifetime (33; 46.5%).
Conclusion: Undertreatment and overtreatment of older adults with cancer are imprecisely defined concepts. We propose new, more rigorous definitions that account for both oncologic factors and geriatric domains.
Figures
References
-
- Shapiro CL. Cancer survivorship. N Engl J Med. 2018;379:2438–2450. - PubMed
-
- Ethun CG, Bilen MA, Jani AB, et al. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J Clin. 2017;67:362–377. - PubMed
-
- Fried TR, Bradley EH, Towle VR, et al. Understanding the treatment preferences of seriously ill patients. N Engl J Med. 2002;346:1061–1066. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
