

Urine Extracellular Vesicle GATA2 mRNA Discriminates Biopsy Result in Men with Suspicion of Prostate Cancer
- PMID: 32250729
- PMCID: PMC7483587
- DOI: 10.1097/JU.0000000000001066
Urine Extracellular Vesicle GATA2 mRNA Discriminates Biopsy Result in Men with Suspicion of Prostate Cancer
Abstract
Purpose: Prostate specific antigen has limited performance in detecting prostate cancer. The transcription factor GATA2 is expressed in aggressive prostate cancer. We analyzed the predictive value of urine extracellular vesicle GATA2 mRNA alone and in combination with a multigene panel to improve detection of prostate cancer and high risk disease.
Materials and methods:
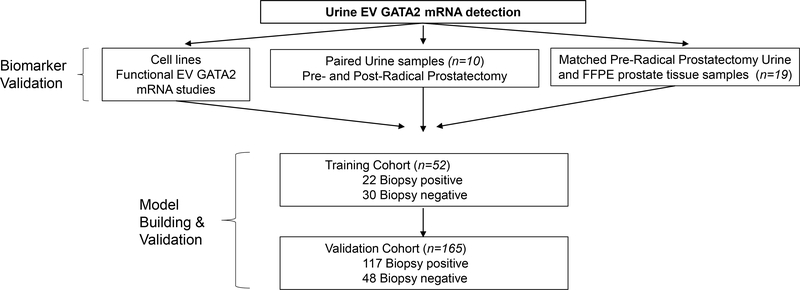
GATA2 mRNA was analyzed in matched extracellular vesicles isolated from urines before and after prostatectomy (16) and paired urine and tissue prostatectomy samples (19). Extracellular vesicle GATA2 mRNA performance to distinguish prostate cancer and high grade disease was tested in training (52) and validation (165) cohorts. The predictive value of a multigene score including
Results:
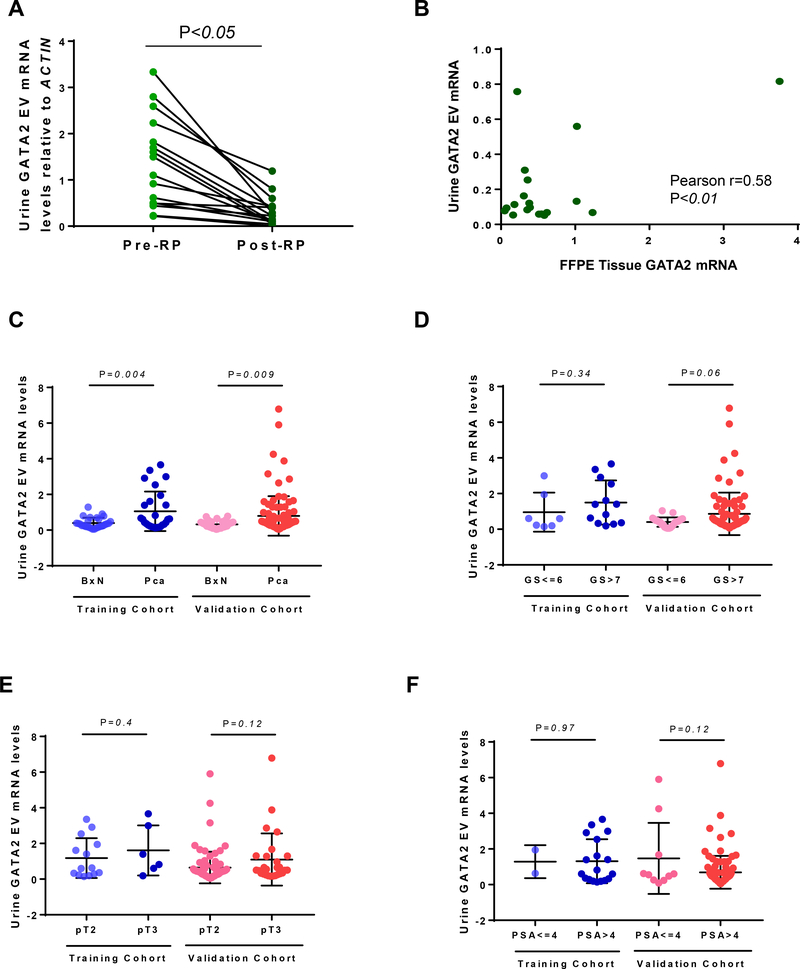
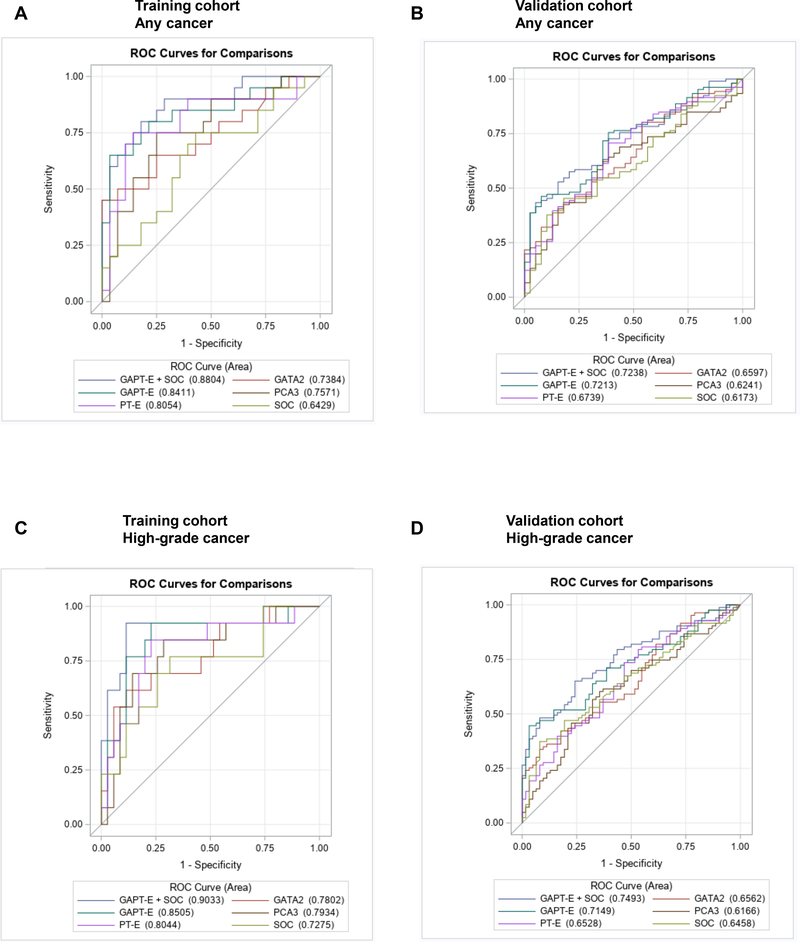
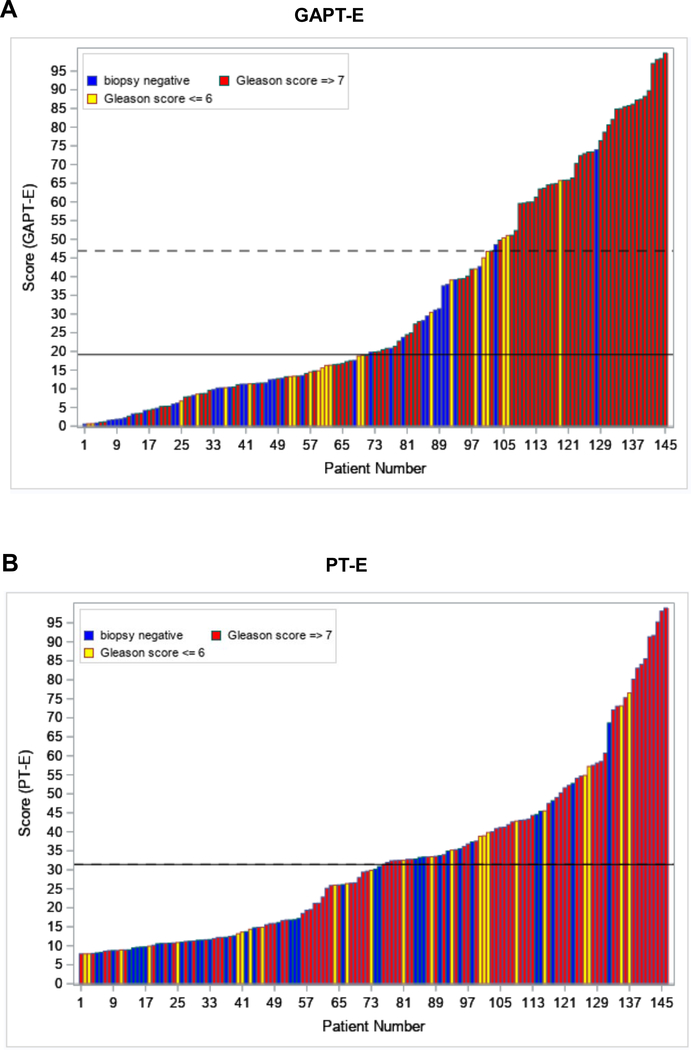
Confirming its prostate origin, urine extracellular vesicle GATA2 mRNA levels decreased significantly after prostatectomy and correlated with prostate cancer tissue GATA2 mRNA levels. In the training and validation cohort GATA2 discriminated prostate cancer (AUC 0.74 and 0.66) and high grade disease (AUC 0.78 and 0.65), respectively. Notably, the GAPT-E score improved discrimination of prostate cancer (AUC 0.84 and 0.72) and high grade cancer (AUC 0.85 and 0.71) in both cohorts when compared with each biomarker alone and PT-E (
Conclusions: Urine extracellular vesicle GATA2 mRNA analysis improves the detection of high risk prostate cancer and may reduce the number of unnecessary biopsies.
Keywords: GATA2 transcription factor; TMPRSS2-ERG fusion protein; extracellular vesicles; human; prostate cancer antigen 3; prostatic neoplasms.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Editorial Comment.J Urol. 2020 Oct;204(4):700. doi: 10.1097/JU.0000000000001066.01. Epub 2020 Jul 30. J Urol. 2020. PMID: 32898984 No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I et al.: Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin, 68: 394, 2018 - PubMed
-
- Potosky AL, Miller BA, Albertsen PC et al.: The role of increasing detection in the rising incidence of prostate cancer. JAMA, 273: 548, 1995 - PubMed
-
- Lavallee LT, Binette A, Witiuk K et al.: Reducing the Harm of Prostate Cancer Screening: Repeated Prostate-Specific Antigen Testing. Mayo Clin Proc, 91: 17, 2016 - PubMed
-
- van Vugt HA, Roobol MJ, Kranse R et al.: Prediction of prostate cancer in unscreened men: external validation of a risk calculator. Eur J Cancer, 47: 903, 2011 - PubMed
-
- Loeb S: Guideline of guidelines: prostate cancer screening. BJU Int, 114: 323, 2014 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
