

Blood-based biomarkers for prediction of intracranial hemorrhage and outcome in patients with moderate or severe traumatic brain injury
- PMID: 32251265
- PMCID: PMC7311234
- DOI: 10.1097/TA.0000000000002706
Blood-based biomarkers for prediction of intracranial hemorrhage and outcome in patients with moderate or severe traumatic brain injury
Abstract
Background: Early identification of traumatic intracranial hemorrhage (ICH) has implications for triage and intervention. Blood-based biomarkers were recently approved by the Food and Drug Administration (FDA) for prediction of ICH in patients with mild traumatic brain injury (TBI). We sought to determine if biomarkers measured early after injury improve prediction of mortality and clinical/radiologic outcomes compared with Glasgow Coma Scale (GCS) alone in patients with moderate or severe TBI (MS-TBI).
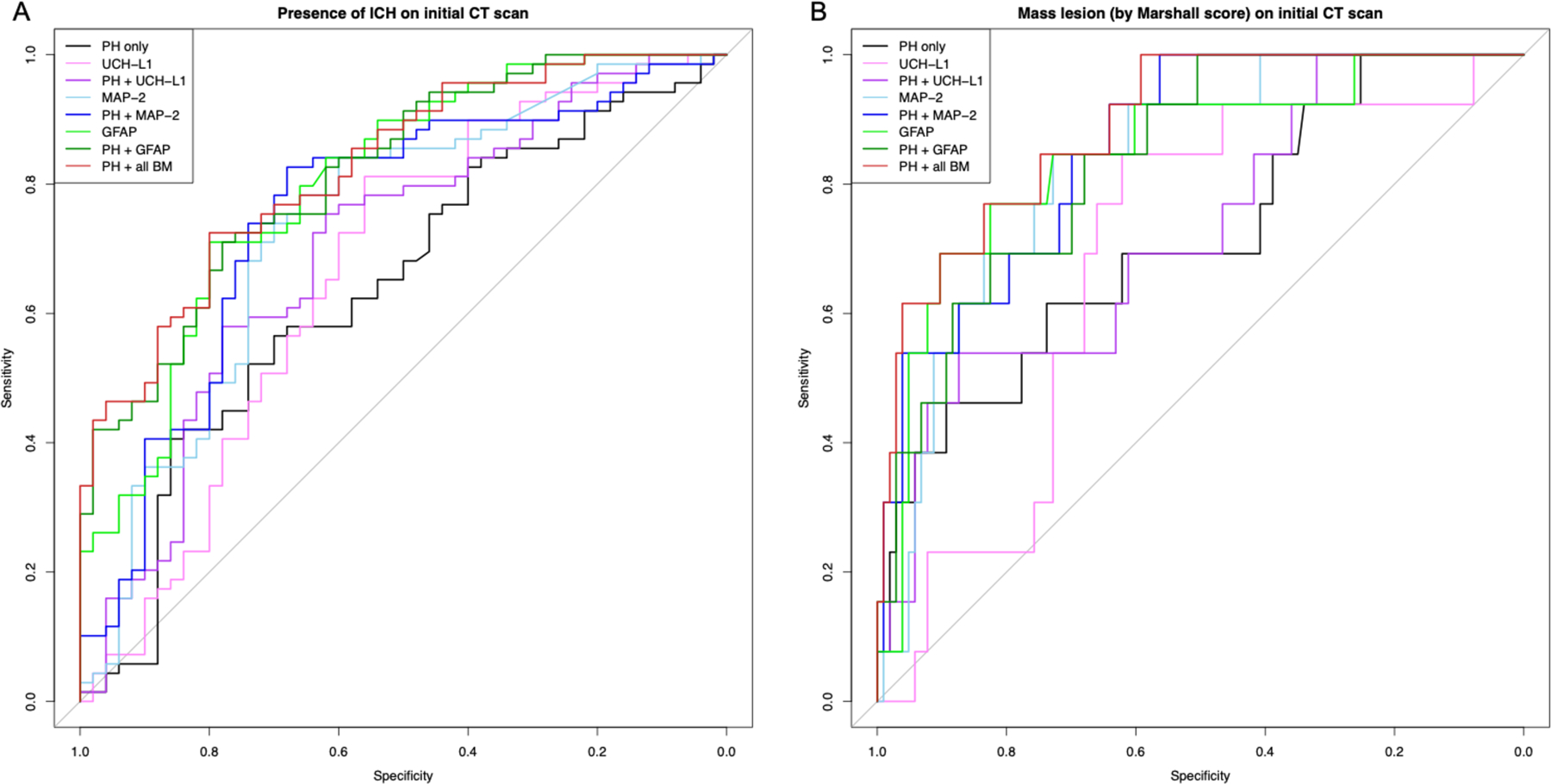
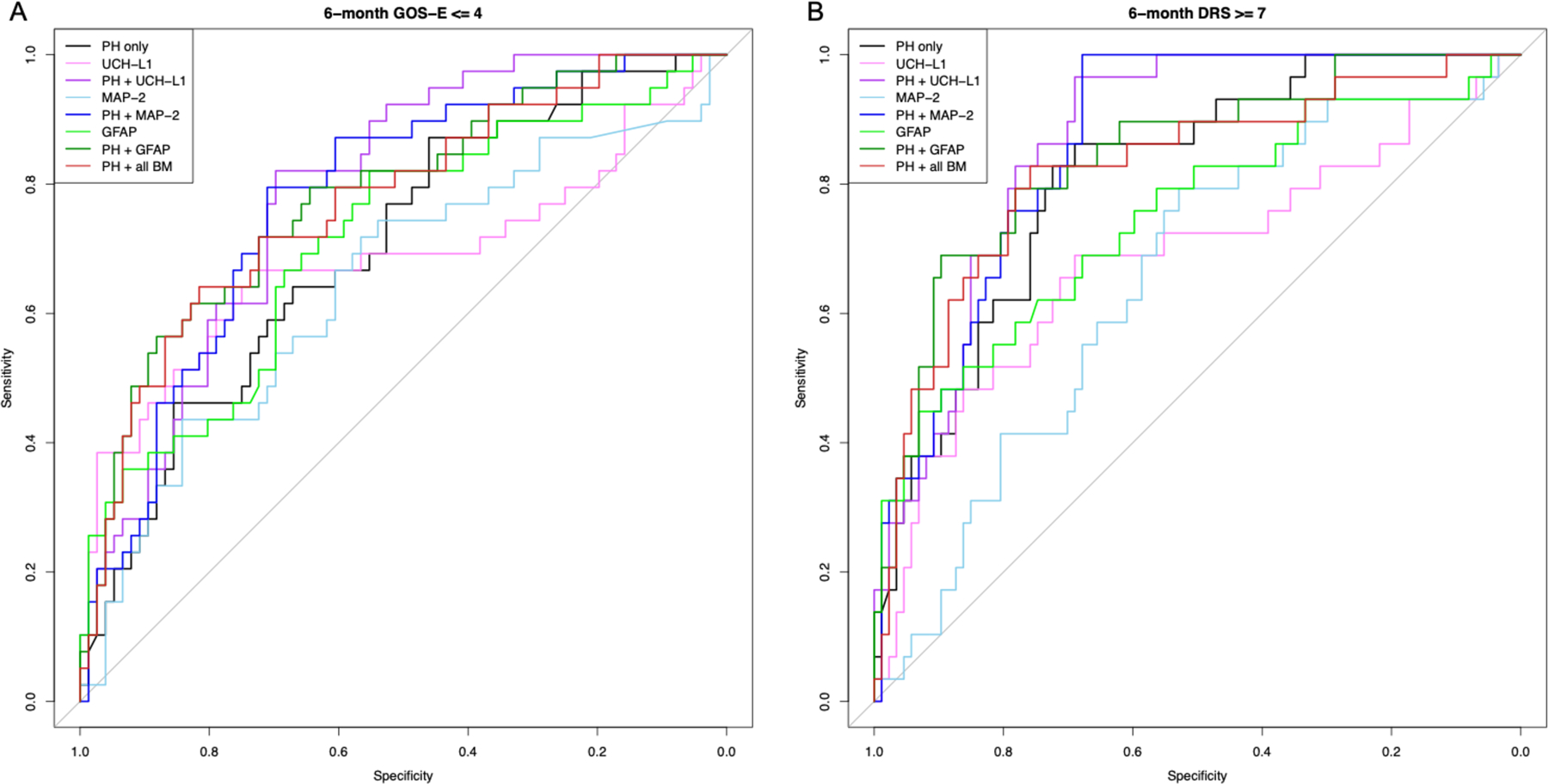
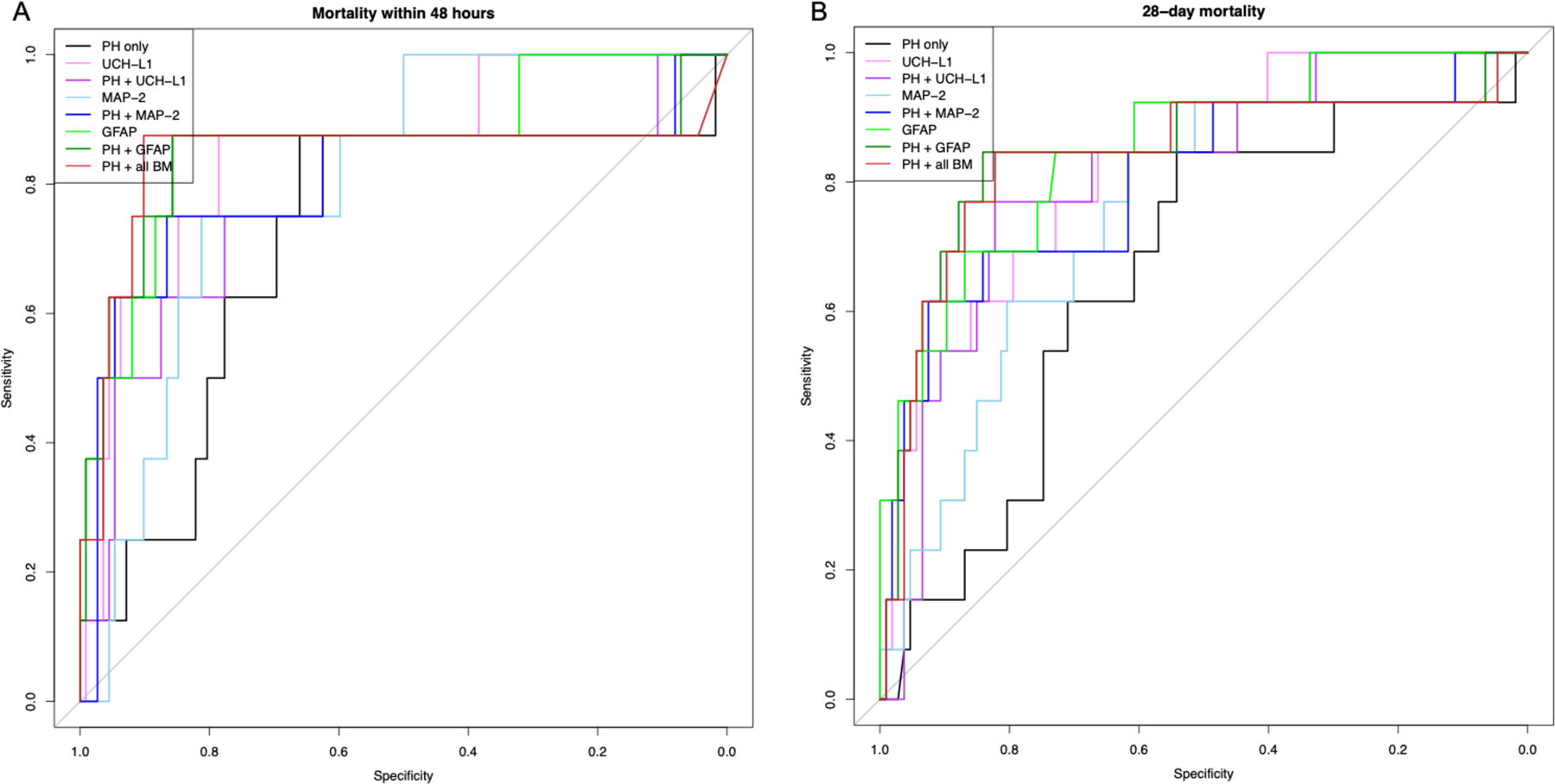
Methods: We measured glial fibrillary acidic protein (GFAP), ubiquitin C-terminal hydrolase L1 (UCH-L1), and microtubule-associated protein-2 (MAP-2) on arrival to the emergency department (ED) in patients with blunt TBI enrolled in the placebo arm of the Prehospital TXA for TBI Trial (prehospital GCS score, 3-12; SPB, > 90). Biomarkers were modeled individually and together with prehospital predictor variables [PH] (GCS score, age, sex). Data were divided into a training data set and test data set for model derivation and evaluation. Models were evaluated for prediction of ICH, mass lesion, 48-hour and 28-day mortality, and 6-month Glasgow Outcome Scale-Extended (GOS-E) and Disability Rating Scale (DRS). Area under the curve (AUC) was evaluated in test data for PH alone, PH + individual biomarkers, and PH + three biomarkers.
Results: Of 243 patients with baseline samples (obtained a median of 84 minutes after injury), prehospital GCS score was 8 (interquartile range, 5-10), 55% had ICH, and 48-hour and 28-day mortality were 7% and 13%, respectively. Poor neurologic outcome at 6 months was observed in 34% based on GOS-E of 4 or less, and 24% based on DRS greater than or equal to7. Addition of each biomarker to PH improved AUC in the majority of predictive models. GFAP+PH compared with PH alone significantly improved AUC in all models (ICH, 0.82 vs. 0.64; 48-hour mortality, 0.84 vs. 0.71; 28-day mortality, 0.84 vs. 0.66; GOS-E, 0.78 vs. 0.69; DRS, 0.84 vs. 0.81, all p < 0.001).
Conclusion: Circulating blood-based biomarkers may improve prediction of neurological outcomes and mortality in patients with MS-TBI over prehospital characteristics alone. Glial fibrillary acidic protein appears to be the most promising. Future evaluation in the prehospital setting is warranted.
Level of evidence: Prospective, Prognostic and Epidemiological, level II.
Figures
References
-
- Frowein RA. Classification of coma. Acta Neurochir (Wien). 1976. March;34(1–4):5–10. - PubMed
-
- Steyerberg EW, Mushkudiani N, Perel P, Butcher I, Lu J, McHugh GS, Murray GD, Marmarou A, Roberts I, Habbema JDF, et al. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. 2008. August 5;5(8):e165. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
