

Review
doi: 10.1038/s41551-020-0525-x.
Epub 2020 Apr 6.
Engineered reproductive tissues
Affiliations
- PMID: 32251392
- PMCID: PMC7416444
- DOI: 10.1038/s41551-020-0525-x
Item in Clipboard
Review
Engineered reproductive tissues
Nat Biomed Eng.
2020 Apr.
Erratum in
-
Author Correction: Engineered reproductive tissues.Nat Biomed Eng. 2020 May;4(5):574. doi: 10.1038/s41551-020-0561-6. Nat Biomed Eng. 2020. PMID: 32332996
Abstract
Engineered male and female biomimetic reproductive tissues are being developed as autonomous in vitro units or as integrated multi-organ in vitro systems to support germ cell and embryo function, and to display characteristic endocrine phenotypic patterns, such as the 28-day human ovulatory cycle. In this Review, we summarize how engineered reproductive tissues facilitate research in reproductive biology, and overview strategies for making engineered reproductive tissues that might eventually allow the restoration of reproductive capacity in patients.
Figures
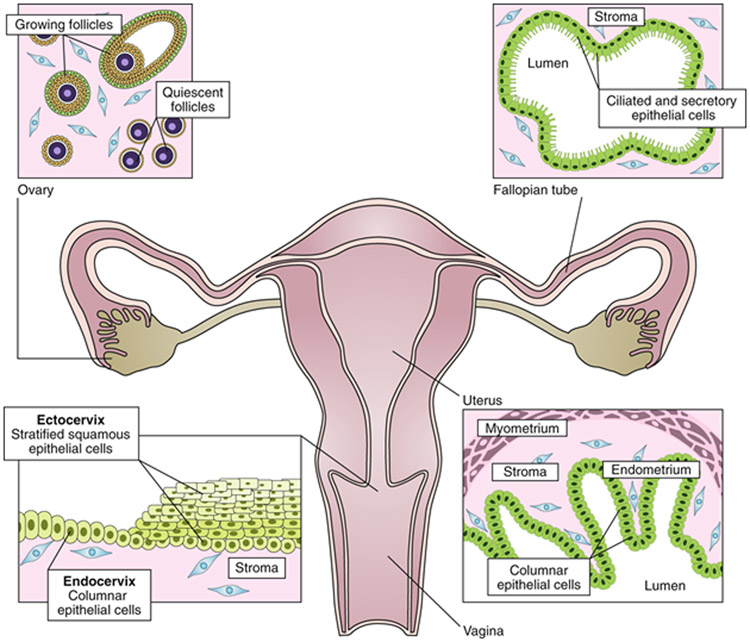
The female reproductive tract consists of the ovaries, fallopian tubes, uterus, cervix and vagina. The ovaries contain follicles—that is, cellular aggregates in which an oocyte is surrounded by hormone-producing granulosa cells. Each month, a cohort of quiescent follicles are activated and begin growth, ultimately resulting in the ovulation of a single oocyte. The oocyte travels through the fallopian tube where the ciliated epithelial cells generate a current that sperm swim against for fertilization. The next organ in the tract is the uterus, where embryo implantation occurs. The muscular layer of the uterus (myometrium) generates contractions. The cervix forms the boundary between the uterus and the vagina. The endocervix resembles the uterus histologically, while the ectocervix is more similar to the vagina. Developing technology for the female reproductive tract requires the understanding of the native tissue and of endocrine interactions.
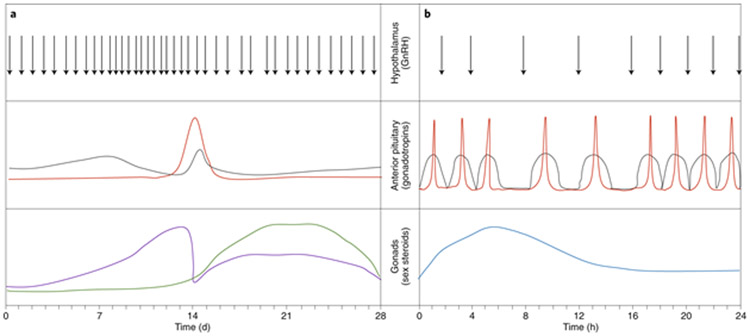
a, The female hypothalamic–pituitary–gonadal axis cycles every 28 d in humans. Pulses of gonadotropin-releasing hormone (GnRH) from the hypothalamus drive the secretion of the gonadotropins FSH (grey) and luteinizing hormone (red) from the anterior pituitary. The gonadotropins instruct the female gonad (that is, the ovary) to produce estradiol (purple) and progesterone (green). b, The male hypothalamic–pituitary–gonadal axis cycles every 24 h in humans. GnRH pulses from the hypothalamus drive the secretion of FSH (grey) and luteinizing hormone (red) from the anterior pituitary. The gonadotropins stimulate production of testosterone (blue) by the Leydig cells of the male gonad (that is, the testis). Engineered reproductive tissue constructs aim to mimic the hormonal changes ex vivo or to restore the complex physiological interactions in vivo.
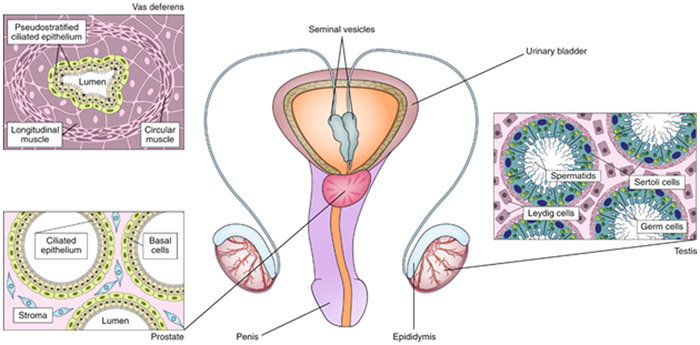
The male reproductive tract consists of the testes, the epididymis, the vas deferens, the seminal vesicles, the prostate and the penis. The testis is composed of seminiferous tubules, which are lined with a layer of germ cells that give rise to spermatids. Within the seminiferous tubules, Sertoli cells support the developing gametes. Leydig cells, located between the tubules, secrete testosterone. The developing sperm travels out of the testis to the epididymis, then to the vas deferens, and is expelled through the penis. The prostate and seminal vesicles secrete fluid that makes up the semen. Engineering reproductive tissue involves the recapitulation of the complex cellular tissue and endocrine relationships that exist in the male reproductive tract towards developing in vitro models or making biomimetic organs for transplantation.
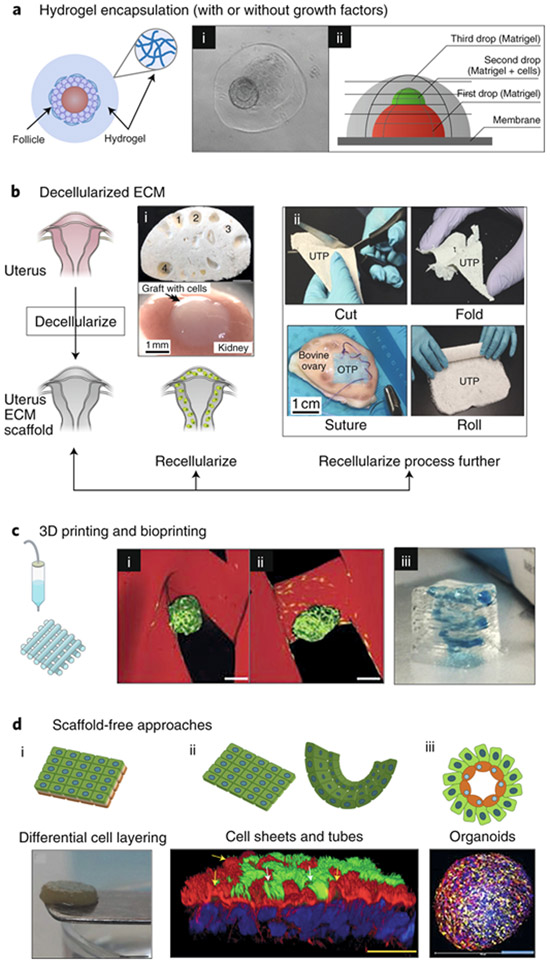
a, Hydrogel encapsulation enables the in vitro culture of ovarian follicles and testicular cells in a manner that mimics their in vivo architecture. (i) 3D structure of the ovarian follicle (arrow) was maintained within collagen–alginate beads. (ii) A three-layer gradient system consisting of testis-cell-containing Matrigel placed between two layers of cell-free Matrigel. The gradient of cells promotes cellular reorganization into functional testicular organoids. b, Decellularization techniques for ovarian, uterine and testis tissues, for both basic research and transplantation. Following decellularization, tissue scaffolds can be (i) directly recellularized or (ii) further processed into other biomaterials. (i) Transplanted decellularized bovine ovary scaffolds (top) seeded with murine ovarian cells (bottom) to restore puberty in ovariectomized mice. The numbers indicate visible pores where large follicles resided and that are maintained following decellularization. (ii) Decellularized composite materials from a variety of organ sources. UTP, bovine uterus ECM; OTP, bovine ovary ECM; CTP, bovine collagen. The composite materials are ideal surgical materials as they can be cut, folded, sutured and rolled, and can support cell adhesion and survival. c, 3D printing and bioprinting provide precise control in the construction of engineered scaffolds for reproductive tissues. (i) 3D-printed bioprosthetic ovaries restore both fertility and endocrine function after transplantation into ovariectomized mice. A tortuous pore network (i) better maintains the ovarian-follicle (green) architecture within the 3D-printed gelatin scaffold (red) compared to a grid-like 90° pore network (ii). Scale bars, 100 μm. (iii) Bioprinted model of the placenta by using human trophoblast cells to study pre-eclampsia. The 3D-printed spiral (blue) resembles the maternal spiral arteries, which trophoblasts invade during normal placentation. d, Scaffold-free approaches, including self-assembling organoids, cell sheets and differential cell layering, have been used to create 3D models of reproductive tissues. (i) Gross appearance of a disk-shaped, scaffold-free 3D cervical stromal equivalent, onto which primary human cervical cells were seeded so as to generate a 3D-human ectocervix model. (ii) Bovine oviduct epithelial cells self-assembled to form floating vesicles with outward facing actively beating cilia (green; indicated by white arrows). Actin filaments appear in red; nuclei appear in blue; yellow arrows indicate primary cilia and actin-rich secretory protrustions. (iii) By using the hanging-drop method, testicular organoids composed of all testicular cell subtypes were created. Spermatogonial stem cells appear in blue, Sertoli cells in yellow and Leydig cells in red.
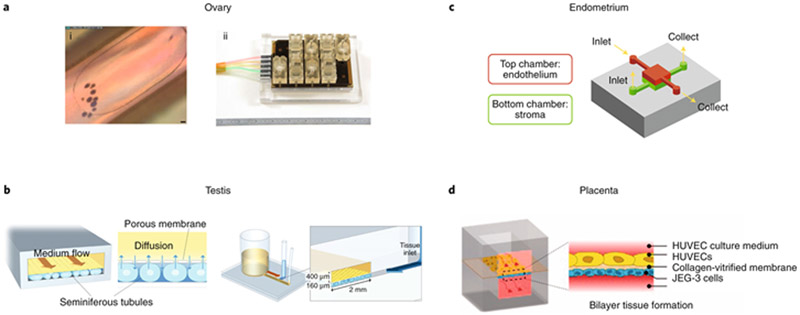
a, The ovary, specifically the follicular microenvironment, can be recreated via microfluidic culture conditions (i; scale bar, 50 μm) within a microphysiological system (ii). The cultures were supplemented with the pituitary hormones FSH and hCG to recreate the estradiol and progesterone profiles of the human 28-d ovulatory cycle. b, A simple two-channel microfluidic device enabled the long-term functional maintenance of ex vivo testis tissue. c, A compartmentalized model of the human endometrium that includes both the endothelium and stroma exhibited a physiological response via prolactin production. d, A two-channel microfluidic system modelled the placental barrier and displayed enhanced mass-transfer dynamics. HUVEC, human umbilical vein endothelial cell.
References
-
- Morris RT The ovarian graft. New York Med. J 62, 436 (1895).
-
- Favre-Inhofer A, Rafii A, Carbonnel M, Revaux A & Ayoubi JM Uterine transplantation: review in human research. J. Gynecol. Obstet. Hum. Reprod 47, 213–221 (2018). - PubMed
-
- Girsdansky J & Newman HF Use of a vitallium testicular implant. Am. J. Surg 53, 514 (1941)
-
- Steptoe PC & Edwards RG Birth after the reimplantation of a human embryo. Lancet 312, 366 (1978) - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
