

Immunosuppressive FK506 treatment leads to more frequent EBV-associated lymphoproliferative disease in humanized mice
- PMID: 32251475
- PMCID: PMC7162544
- DOI: 10.1371/journal.ppat.1008477
Immunosuppressive FK506 treatment leads to more frequent EBV-associated lymphoproliferative disease in humanized mice
Erratum in
-
Correction: Immunosuppressive FK506 treatment leads to more frequent EBV-associated lymphoproliferative disease in humanized mice.PLoS Pathog. 2020 Dec 21;16(12):e1009167. doi: 10.1371/journal.ppat.1009167. eCollection 2020 Dec. PLoS Pathog. 2020. PMID: 33347498 Free PMC article.
Abstract
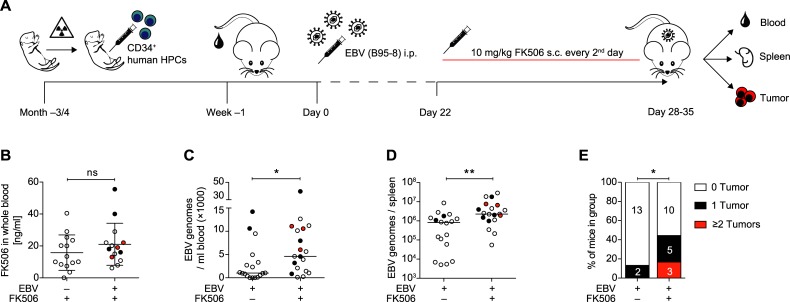
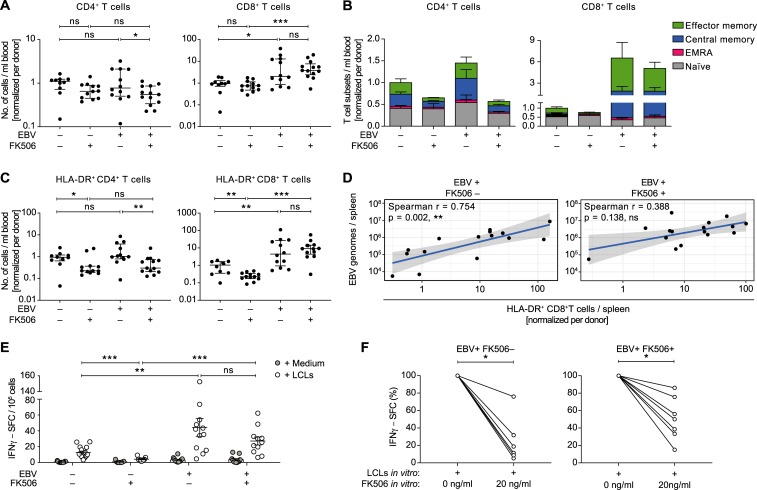
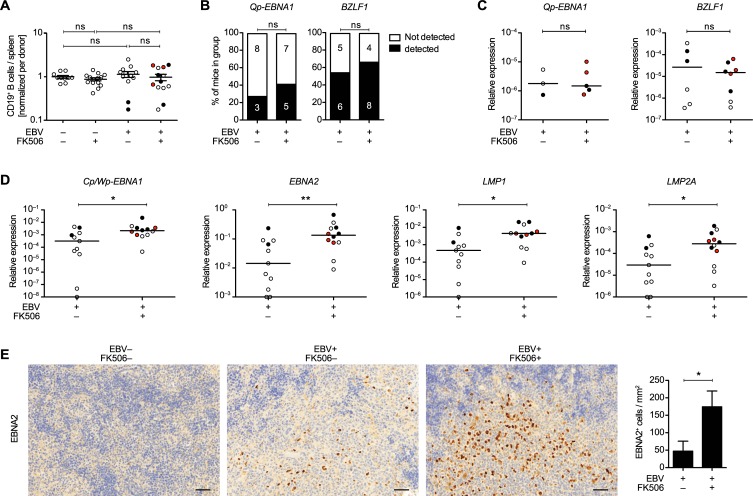
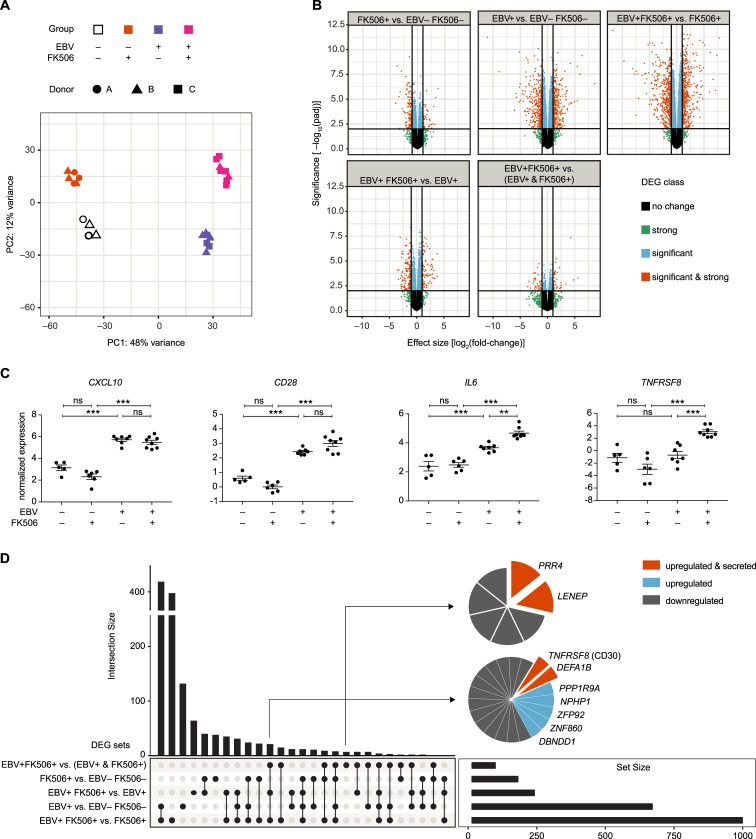
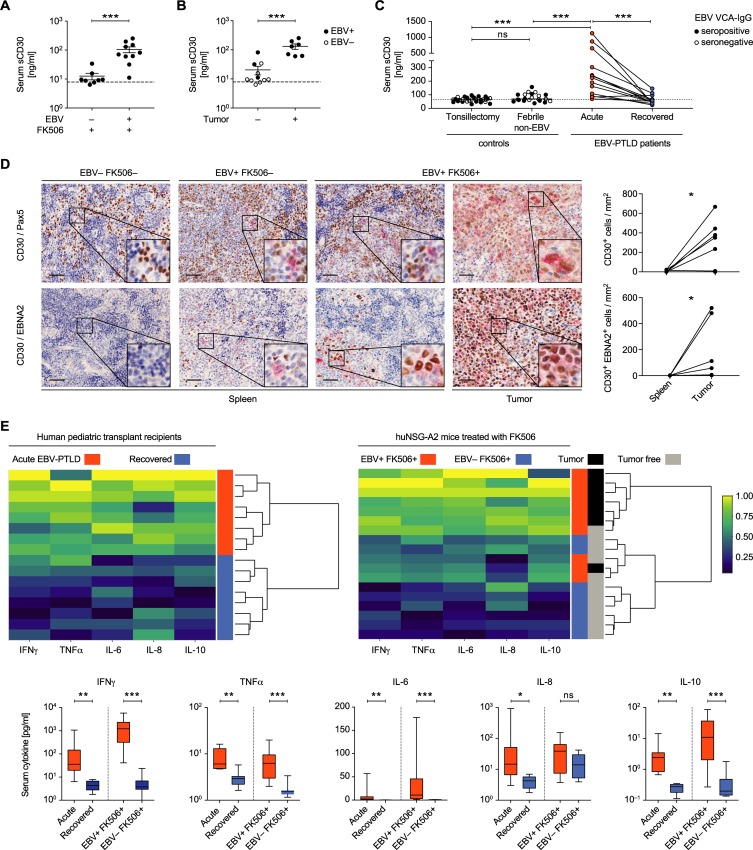
Post-transplant lymphoproliferative disorder (PTLD) is a potentially fatal complication after organ transplantation frequently associated with the Epstein-Barr virus (EBV). Immunosuppressive treatment is thought to allow the expansion of EBV-infected B cells, which often express all eight oncogenic EBV latent proteins. Here, we assessed whether HLA-A2 transgenic humanized NSG mice treated with the immunosuppressant FK506 could be used to model EBV-PTLD. We found that FK506 treatment of EBV-infected mice led to an elevated viral burden, more frequent tumor formation and diminished EBV-induced T cell responses, indicative of reduced EBV-specific immune control. EBV latency III and lymphoproliferation-associated cellular transcripts were up-regulated in B cells from immunosuppressed animals, akin to the viral and host gene expression pattern found in EBV-PTLD. Utilizing an unbiased gene expression profiling approach, we identified genes differentially expressed in B cells of EBV-infected animals with and without FK506 treatment. Upon investigating the most promising candidates, we validated sCD30 as a marker of uncontrolled EBV proliferation in both humanized mice and in pediatric patients with EBV-PTLD. High levels of sCD30 have been previously associated with EBV-PTLD in patients. As such, we believe that humanized mice can indeed model aspects of EBV-PTLD development and may prove useful for the safety assessment of immunomodulatory therapies.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Co-infection of Cytomegalovirus and Epstein-Barr Virus Diminishes the Frequency of CD56dimNKG2A+KIR- NK Cells and Contributes to Suboptimal Control of EBV in Immunosuppressed Children With Post-transplant Lymphoproliferative Disorder.Front Immunol. 2020 Jun 17;11:1231. doi: 10.3389/fimmu.2020.01231. eCollection 2020. Front Immunol. 2020. PMID: 32625211 Free PMC article.
-
The Immune Response to Epstein Barr Virus and Implications for Posttransplant Lymphoproliferative Disorder.Transplantation. 2017 Sep;101(9):2009-2016. doi: 10.1097/TP.0000000000001767. Transplantation. 2017. PMID: 28376031 Free PMC article. Review.
-
The Epstein-Barr virus and post-transplant lymphoproliferative disease: interplay of immunosuppression, EBV, and the immune system in disease pathogenesis.Transpl Infect Dis. 2001 Jun;3(2):60-9. doi: 10.1034/j.1399-3062.2001.003002060.x. Transpl Infect Dis. 2001. PMID: 11395971 Review.
-
EBV-positive mucocutaneous ulcer in organ transplant recipients: a localized indolent posttransplant lymphoproliferative disorder.Am J Surg Pathol. 2014 Nov;38(11):1522-9. doi: 10.1097/PAS.0000000000000282. Am J Surg Pathol. 2014. PMID: 25007145
-
Relationship of immunosuppression to Epstein-Barr viral load and lymphoproliferative disease in pediatric heart transplant patients.J Heart Lung Transplant. 2008 Jan;27(1):100-5. doi: 10.1016/j.healun.2007.09.027. J Heart Lung Transplant. 2008. PMID: 18187094
Cited by
-
Co-infection of Cytomegalovirus and Epstein-Barr Virus Diminishes the Frequency of CD56dimNKG2A+KIR- NK Cells and Contributes to Suboptimal Control of EBV in Immunosuppressed Children With Post-transplant Lymphoproliferative Disorder.Front Immunol. 2020 Jun 17;11:1231. doi: 10.3389/fimmu.2020.01231. eCollection 2020. Front Immunol. 2020. PMID: 32625211 Free PMC article.
-
Roles of Lytic Viral Replication and Co-Infections in the Oncogenesis and Immune Control of the Epstein-Barr Virus.Cancers (Basel). 2021 May 10;13(9):2275. doi: 10.3390/cancers13092275. Cancers (Basel). 2021. PMID: 34068598 Free PMC article. Review.
-
Modification of EBV Associated Lymphomagenesis and Its Immune Control by Co-Infections and Genetics in Humanized Mice.Front Immunol. 2021 Mar 23;12:640918. doi: 10.3389/fimmu.2021.640918. eCollection 2021. Front Immunol. 2021. PMID: 33833760 Free PMC article. Review.
-
EBV renders B cells susceptible to HIV-1 in humanized mice.Life Sci Alliance. 2020 Jun 23;3(8):e202000640. doi: 10.26508/lsa.202000640. Print 2020 Aug. Life Sci Alliance. 2020. PMID: 32576602 Free PMC article.
-
KSHV infection of B cells primes protective T cell responses in humanized mice.Nat Commun. 2024 Jun 6;15(1):4841. doi: 10.1038/s41467-024-49209-w. Nat Commun. 2024. PMID: 38844783 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
