

Pembrolizumab for management of patients with NSCLC and brain metastases: long-term results and biomarker analysis from a non-randomised, open-label, phase 2 trial
- PMID: 32251621
- PMCID: PMC7380514
- DOI: 10.1016/S1470-2045(20)30111-X
Pembrolizumab for management of patients with NSCLC and brain metastases: long-term results and biomarker analysis from a non-randomised, open-label, phase 2 trial
Abstract
Background: We did a phase 2 trial of pembrolizumab in patients with non-small-cell lung cancer (NSCLC) or melanoma with untreated brain metastases to determine the activity of PD-1 blockade in the CNS. Interim results were previously published, and we now report an updated analysis of the full NSCLC cohort.
Methods: This was an open-label, phase 2 study of patients from the Yale Cancer Center (CT, USA). Eligible patients were at least 18 years of age with stage IV NSCLC with at least one brain metastasis 5-20 mm in size, not previously treated or progressing after previous radiotherapy, no neurological symptoms or corticosteroid requirement, and Eastern Cooperative Oncology Group performance status less than two. Modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria was used to evaluate CNS disease; systemic disease was not required for participation. Patients were treated with pembrolizumab 10 mg/kg intravenously every 2 weeks. Patients were in two cohorts: cohort 1 was for those with PD-L1 expression of at least 1% and cohort 2 was patients with PD-L1 less than 1% or unevaluable. The primary endpoint was the proportion of patients achieving a brain metastasis response (partial response or complete response, according to mRECIST). All treated patients were analysed for response and safety endpoints. This study is closed to accrual and is registered with ClinicalTrials.gov, NCT02085070.
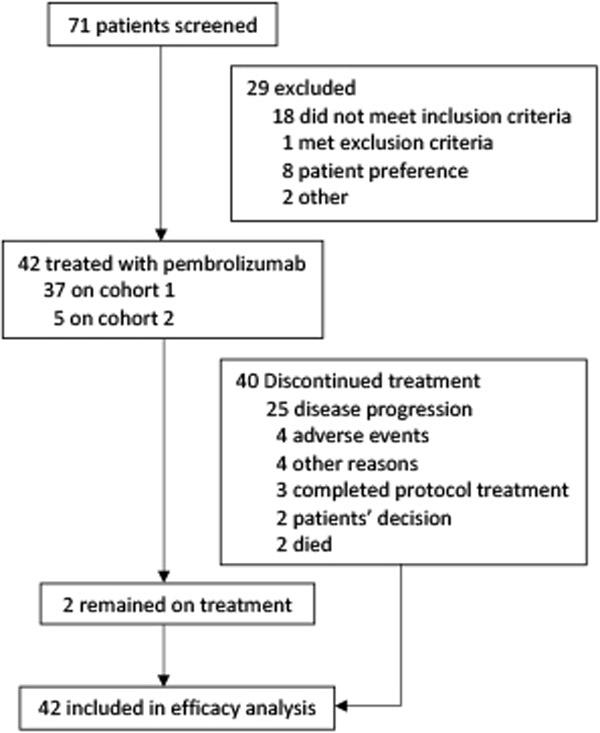
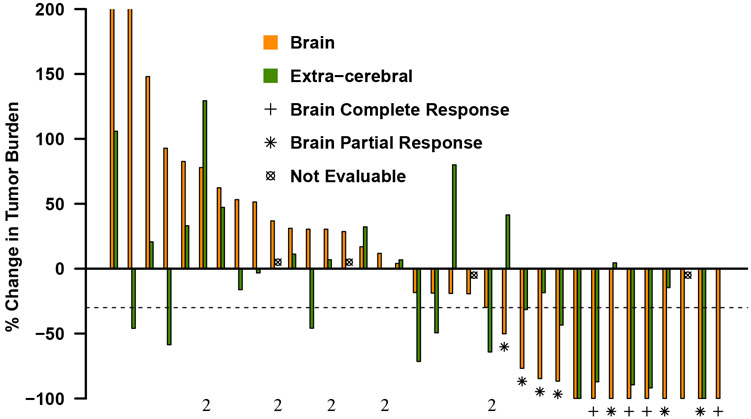
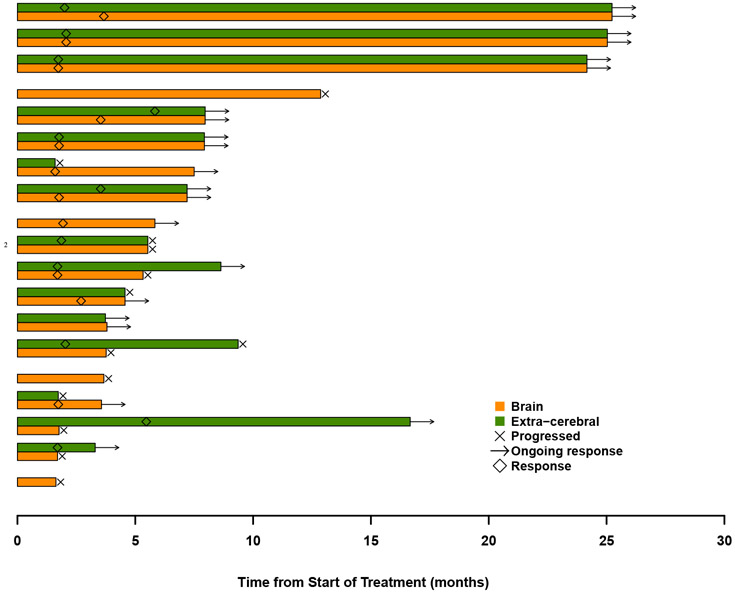
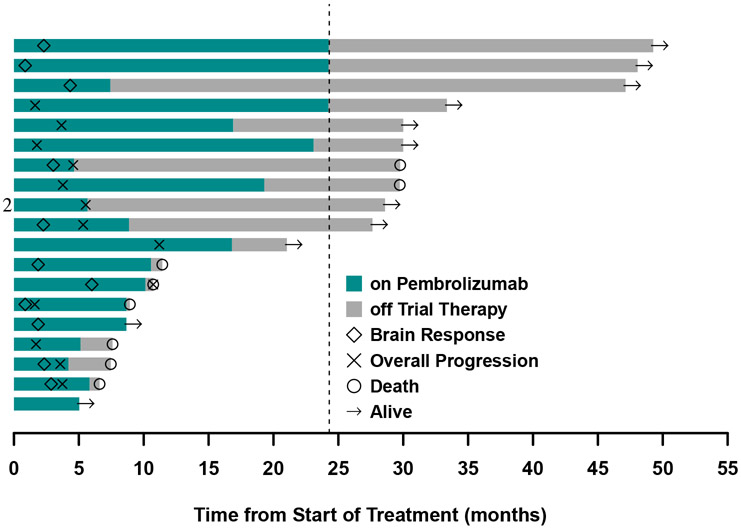
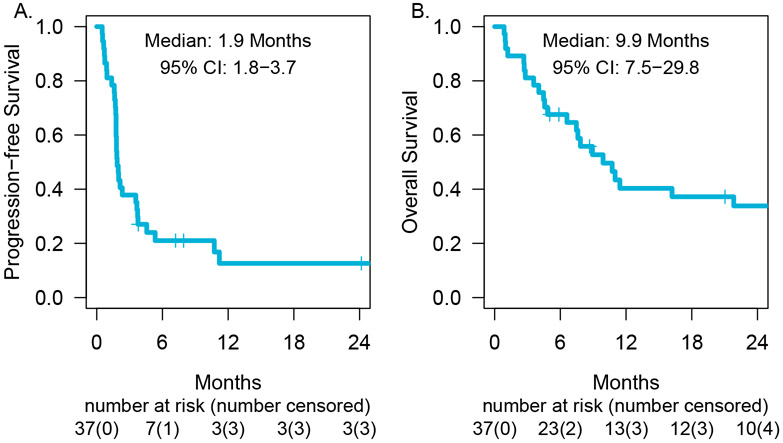
Findings: Between March 31, 2014, and May 21, 2018, 42 patients were treated. Median follow-up was 8·3 months (IQR 4·5-26·2). 11 (29·7% [95% CI 15·9-47·0]) of 37 patients in cohort 1 had a brain metastasis response. There were no responses in cohort 2. Grade 3-4 adverse events related to treatment included two patients with pneumonitis, and one each with constitutional symptoms, colitis, adrenal insufficiency, hyperglycaemia, and hypokalaemia. Treatment-related serious adverse events occurred in six (14%) of 42 patients and were pneumonitis (n=2), acute kidney injury, colitis, hypokalaemia, and adrenal insufficiency (n=1 each). There were no treatment-related deaths.
Interpretation: Pembrolizumab has activity in brain metastases from NSCLC with PD-L1 expression at least 1% and is safe in selected patients with untreated brain metastases. Further investigation of immunotherapy in patients with CNS disease from NSCLC is warranted.
Funding: Merck and the Yale Cancer Center.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests:
SBG reports grants from Merck during the conduct of the study and grants from AstraZeneca and Boehringer Ingelheim and personal fees from AstraZeneca, Eli Lilly, Bristol-Myers Squibb, Boehringer Ingelheim, Genentech, Amgen and Spectrum outside the submitted work. KAS reports personal fees from Clinica Alemana Santiago, Celgene, Moderna Therapeutics, Shattuck Labs, Pierre-Fabre, Astrazeneca, Dyanamo Therapeutics, EMD Serono, Abbvie, Agenus, Torque Therapeutics. Research funding from: Navigate Bipharma (Novartis), Vasculox/Tioma, Tesaro, Moderna Therapeutics, Takeda Pharmaceuticals, Surface Oncology, Pierre-Fabre Research Institute, Merck, Bristol-Myers Squibb, AstraZeneca and Eli Lilly outside the submitted work. SNG reports Research Support to Institution (Yale) and consultant to Bristol-Myers Squibb, consultant to NEKTAR, Research funding (to Yale) from Genentech/Roche, Research funding (to Yale) from Iovance outside the submitted work. RSH is a member of the board of directors (non-executive/ independent) for Junshi Pharmaceuticals and reports grants from AstraZeneca, Eli Lilly and Company, Merck and Company and personal fees from Abbvie Pharmaceuticals, ARMO Biosciences, AstraZeneca, Biodesix, Bolt Biotherapeutics, Bristol-Myers Squibb, Eli Lilly and Company, EMD Serrano, Genentech/Roche, Genmab, Halozyme, Heat Biologics, IMAB Biopharma, Immunocore, Infinity Pharmaceuticals, Loxo Oncology, Merck and Company, Midas Health Analytics, Nektar, Neon Therapeutics, NextCure, Novartis, Pfizer, Sanofi, Seattle Genetics, Shire PLC, Spectrum Pharmaceuticals, Symphogen, Takeda, Tesaro, Tocagen outside the submitted work. AC reports grants from Bristol-Myers Squibb, Abbvie, AstraZeneca, and Amgen and personal fees from AstraZeneca, Bristol-Myers Squibb, Abbvie, Boehringer-Ingelheim, and Genentech/Roche outside the submitted work. RL reports personal fees from AstraZeneca outside the submitted work. FHW reports grants from Agios and personal fees from Loxo Oncology outside the submitted work. JY reports personal fees from Augmenix / Boston Scientific and Galera Pharmaceuticals outside the submitted work. YK reports grants from Merck during the conduct of the study and grants from Bristol-Myers Squibb and Apexigen and personal fees from Alexion, Corvus, Nektar, Biodesix, Roche-Genentech, Pfizer, Iovance, Immunocore, Celldex, and Array Biopharma, outside the submitted work. VC reports personal fees from Monteris Medical Inc, MRI Interventions, and Brainlab AG outside the submitted work. HMK reports grants from Merck during the conduct of the study and grants from Bristol-Myers Squibb and Apexigen and personal fees from Alexion, Corvus, Nektar, Biodesix, Roche-Genentech, Pfizer, Iovance, Immunocore, Celldex, and Array Biopharma, outside the submitted work. AM, SBO, LJ, TT, KP, ER, HG, AK, RG, HW, MR, GZ, and WW have no conflicts to report.
Figures
References
-
- Reungwetwattana T, Nakagawa K, Cho BC, et al. CNS Response to Osimertinib Versus Standard Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors in Patients With Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. J Clin Oncol 2018: JCO2018783118. - PubMed
-
- Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med 2016; 375(19): 1823–33. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
