

Physical Fitness and Self-Rated Health in Children and Adolescents: Cross-Sectional and Longitudinal Study
- PMID: 32252318
- PMCID: PMC7177446
- DOI: 10.3390/ijerph17072413
Physical Fitness and Self-Rated Health in Children and Adolescents: Cross-Sectional and Longitudinal Study
Abstract
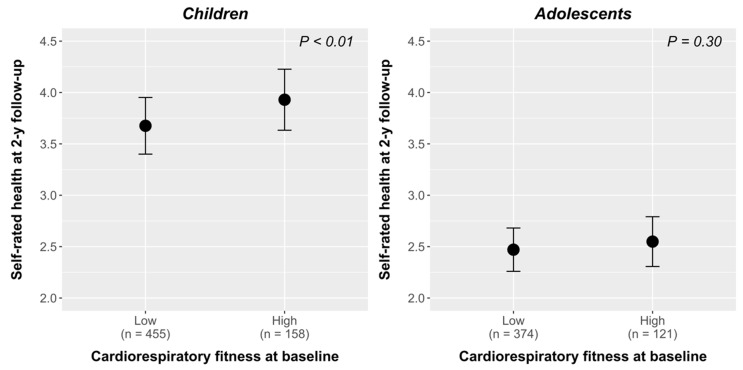
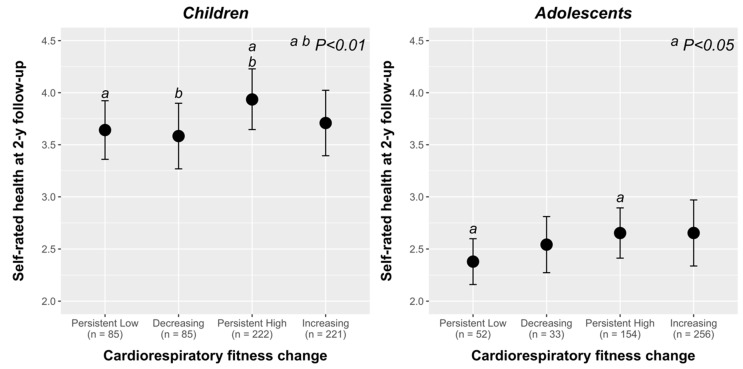
Self-rated health (SRH) is an independent determinant for all-cause mortality. We aimed to examine the independent and combined associations of components of physical fitness with SRH at baseline (cross-sectional) and two years later (longitudinal) in children and adolescents. Spanish youth (N = 1378) aged 8 to 17.9 years participated at baseline. The dropout rate at 2-year follow-up was 19.5% (n = 270). Participants were categorized as either children (8 to 11.9 years age) or adolescents (12 to 17.9 years age). The ALPHA health- related fitness test battery for youth was used to assess physical fitness, and SRH was measured by a single-item question. Cumulative link, ANOVA and ANCOVA models were fitted to analyze the data. Cardiorespiratory fitness, relative upper body isometric muscular strength, muscular strength score, and global physical fitness were positively associated with SRH in children (OR, 1.048; 95% CI, 1.020-1.076; OR, 18.921; 95% CI, 3.47-104.355; OR, 1.213; 95% CI, 1.117-1.319, and OR, 1.170; 95% CI, 1.081-1.266, respectively; all p < 0.001) and adolescents (OR, 1.057; 95% CI, 1.037-1.076; OR, 5.707; 95% CI, 1.122-29.205; OR, 1.169; 95% CI, 1.070-1.278, and OR, 1.154 95% CI, 1.100-1.210, respectively; all p < 0.001); and motor fitness was positively associated with SRH only in adolescents at baseline (OR, 1.192; 95% CI, 1.066-1.309; p < 0.01). Cardiorespiratory fitness and global physical fitness were positively associated with SRH in children two years later (OR, 1.056; 95% CI, 1.023-1.091; p < 0.001; and OR, 1.082; 95% CI, 1.031-1.136; p < 0.01; respectively). Only cardiorespiratory fitness was independently associated with SRH in children and adolescents at baseline (OR, 1.059; 95% CI, 1.029-1.090; and OR, 1.073; 95% CI, 1.050-1.097, respectively; both p < 0.001) and two years later (OR, 1.075; 95% CI, 1.040-1.112; p < 0.001; and OR, 1.043; 95% CI, 1.014-1.074; p < 0.01, respectively). A high level of cardiorespiratory fitness at baseline or maintaining high levels of cardiorespiratory fitness from the baseline to 2-year follow-up were associated with a higher level of SRH at 2-year follow-up in children (p < 0.01) and adolescents (p < 0.05). These findings emphasize the importance of cardiorespiratory fitness as strong predictor of present and future SRH in youth. Intervention programs to enhance cardiorespiratory fitness level of the youth population are urgently needed for present and future youth's health.
Keywords: cardiorespiratory fitness; children and adolescents; motor fitness; muscular strength; physical fitness; self-rated health.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Physical fitness and psychological health in overweight/obese children: A cross-sectional study from the ActiveBrains project.J Sci Med Sport. 2018 Feb;21(2):179-184. doi: 10.1016/j.jsams.2017.09.019. Epub 2017 Oct 4. J Sci Med Sport. 2018. PMID: 29031643
-
Predictive value of physical fitness on self-rated health: A longitudinal study.Scand J Med Sci Sports. 2021 Apr;31 Suppl 1:56-64. doi: 10.1111/sms.13841. Scand J Med Sci Sports. 2021. PMID: 33038037
-
Muscle Fitness Cut Points for Early Assessment of Cardiovascular Risk in Children and Adolescents.J Pediatr. 2019 Mar;206:134-141.e3. doi: 10.1016/j.jpeds.2018.10.026. Epub 2018 Nov 7. J Pediatr. 2019. PMID: 30413315
-
An Update on Secular Trends in Physical Fitness of Children and Adolescents from 1972 to 2015: A Systematic Review.Sports Med. 2021 Feb;51(2):303-320. doi: 10.1007/s40279-020-01373-x. Sports Med. 2021. PMID: 33159655 Free PMC article.
-
Effects of different supervised and structured physical exercise on the physical fitness trainability of children and adolescents: a meta-analysis and meta-regression : Physical fitness trainability in children and adolescents' health.BMC Pediatr. 2024 Dec 5;24(1):798. doi: 10.1186/s12887-024-04929-2. BMC Pediatr. 2024. PMID: 39639233 Free PMC article.
Cited by
-
Exploring the self-reported physical fitness and self-rated health, mental health disorders, and body satisfaction among Chinese adolescents: A cross-sectional study.Front Psychol. 2022 Sep 15;13:1003231. doi: 10.3389/fpsyg.2022.1003231. eCollection 2022. Front Psychol. 2022. PMID: 36186394 Free PMC article.
-
Primary school children's health and its association with physical fitness development and health-related factors.AIMS Public Health. 2023 Dec 4;11(1):1-18. doi: 10.3934/publichealth.2024001. eCollection 2024. AIMS Public Health. 2023. PMID: 38617409 Free PMC article.
-
Research on the effect of different aerobic activity on physical fitness and executive function in primary school students.Sci Rep. 2024 Apr 4;14(1):7956. doi: 10.1038/s41598-024-58009-7. Sci Rep. 2024. PMID: 38575618 Free PMC article.
-
Reference centiles based on year-to-year changes for a longitudinal evaluation of motor performance in children and adolescents.PLoS One. 2022 Jan 7;17(1):e0262163. doi: 10.1371/journal.pone.0262163. eCollection 2022. PLoS One. 2022. PMID: 34995341 Free PMC article.
-
Physical activity, physical fitness and self-rated health: cross-sectional and longitudinal associations in adolescents.BMJ Open Sport Exerc Med. 2024 Mar 29;10(1):e001642. doi: 10.1136/bmjsem-2023-001642. eCollection 2024. BMJ Open Sport Exerc Med. 2024. PMID: 38562154 Free PMC article.
References
-
- Heard H.E., Gorman B.K., Kapinus C.A. Family Structure and Self-Rated Health in Adolescence and Young Adulthood. Popul. Res. Policy Rev. 2008;27:773. doi: 10.1007/s11113-008-9090-9. - DOI
