

Immunohistochemical Results of Soft tissues Around a New Implant Healing-Abutment Surface: A Human Study
- PMID: 32252463
- PMCID: PMC7230724
- DOI: 10.3390/jcm9041009
Immunohistochemical Results of Soft tissues Around a New Implant Healing-Abutment Surface: A Human Study
Abstract
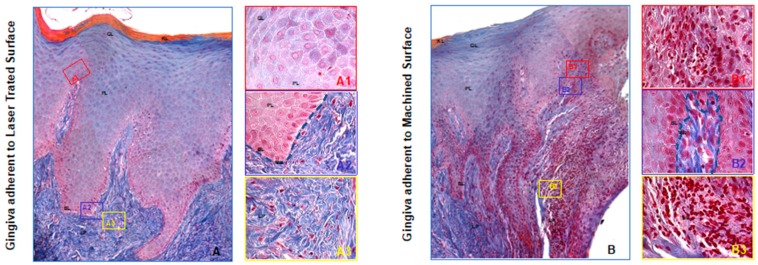
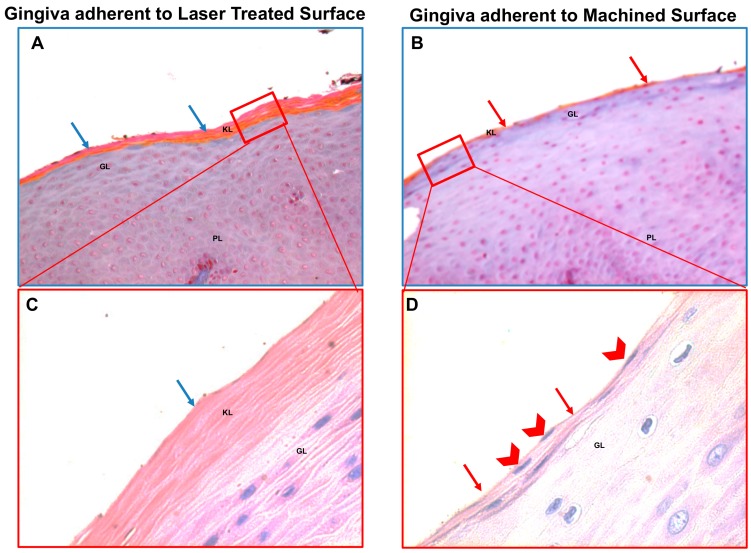
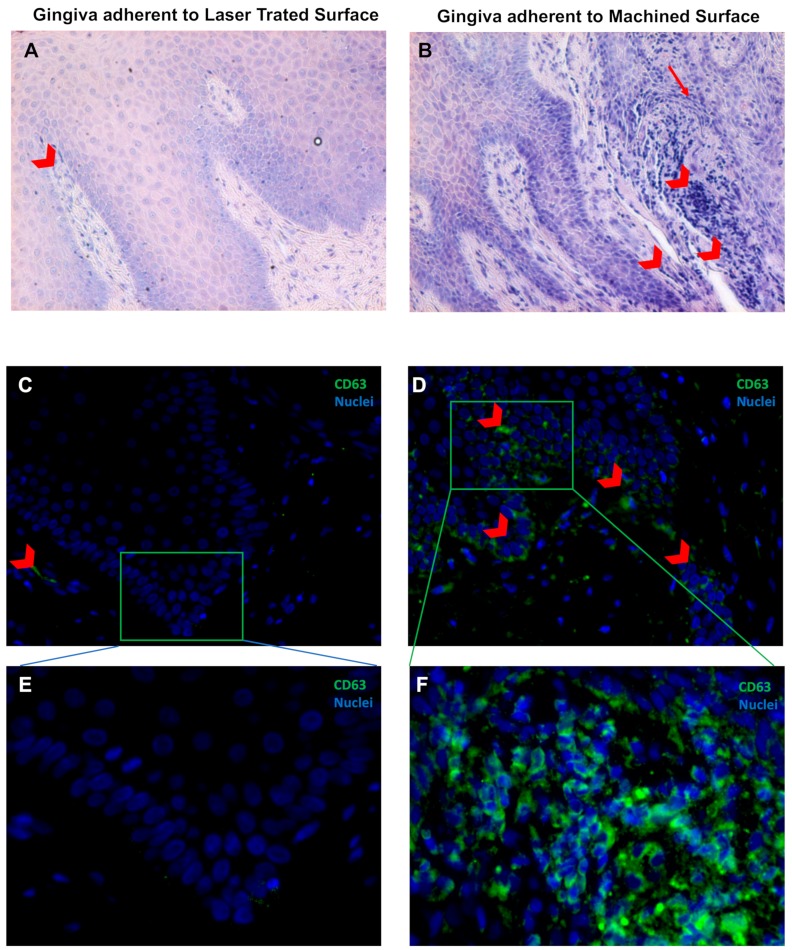
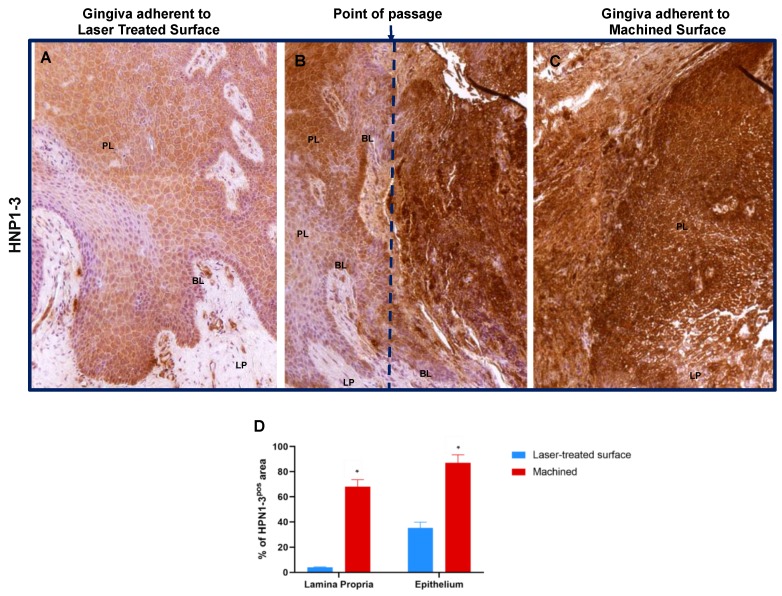
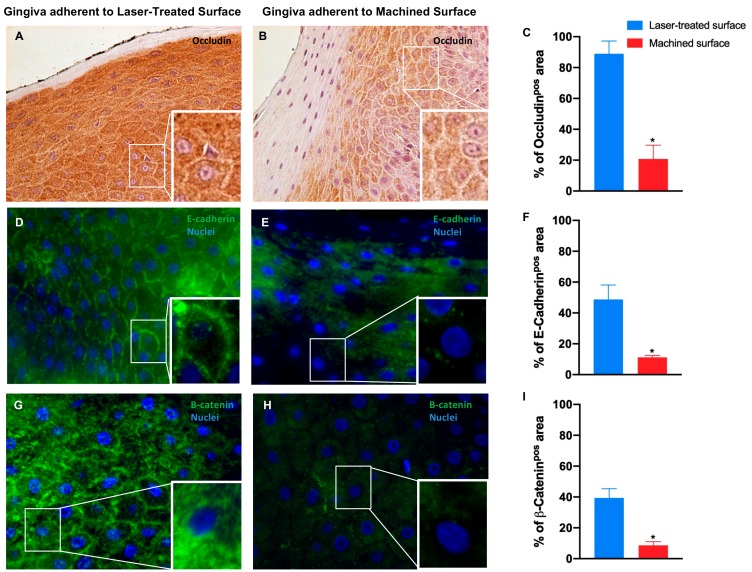
Although, the high success rate of implant rehabilitation treatment, the biological complications such as bone loss and peri-implantitis are still present. The creation of a coronal biological seal between the implant and the oral tissues seems to be a crucial point on preserving dental implants. The objective of this study was to immunohistochemically analyze the behavior of peri-implant soft tissues around a new implant healing-abutment surface on humans. A total of 30 soft tissue biopsies were collected after a healing period of 30 (±7) days, to analyze the expression of inflammatory (cluster of differentiation 63 (CD63), human neutrophil peptides 1-3 (HPN1-3)) and junctional (E-cadherin, occludin, and β-catenin) markers, on soft tissues around laser treated and machined alternated healing abutments. The evaluation demonstrated the whole area of the soft tissues adherent to the laser treated surface with a regular morphology. While several stress hallmarks in correspondence of machined surfaces were shown such as: a) An irregular, disrupted, and discontinued basal membrane with an increased inflammation evident both the epithelial and connective tissues; b) the absence or defective proper keratinization process of the external layer, and c) damages in the cell to cell interaction. In conclusion, the laser treated surface is preferable to maintain the integrity and functionality of the gingiva epithelium.
Keywords: dental implant; immunohistochemical analysis; implant surface; laser treated; peri-implant soft tissues.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Moraschini V., Poubel L.A., Ferreira V.F., Barboza Edos S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015;44:377–388. doi: 10.1016/j.ijom.2014.10.023. - DOI - PubMed
-
- Misch C.E., Perel M.L., Wang H.L., Sammartino G., Galindo-Moreno P., Trisi P., Steigmann M., Rebaudi A., Palti A., Pikos M.A., et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008;17:5–15. doi: 10.1097/ID.0b013e3181676059. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
