

Fetal Aortic Valvuloplasty for Evolving Hypoplastic Left Heart Syndrome: A Decision Analysis
- PMID: 32252549
- PMCID: PMC7737668
- DOI: 10.1161/CIRCOUTCOMES.119.006127
Fetal Aortic Valvuloplasty for Evolving Hypoplastic Left Heart Syndrome: A Decision Analysis
Abstract
Background: Fetal aortic valvuloplasty (FAV) may prevent progression of midgestation aortic stenosis to hypoplastic left heart syndrome. However, FAV has well-established risks, and its survival benefit remains unknown. Our primary aim was to determine whether FAV for midgestation aortic stenosis increases survival from fetal diagnosis to age 6 years.
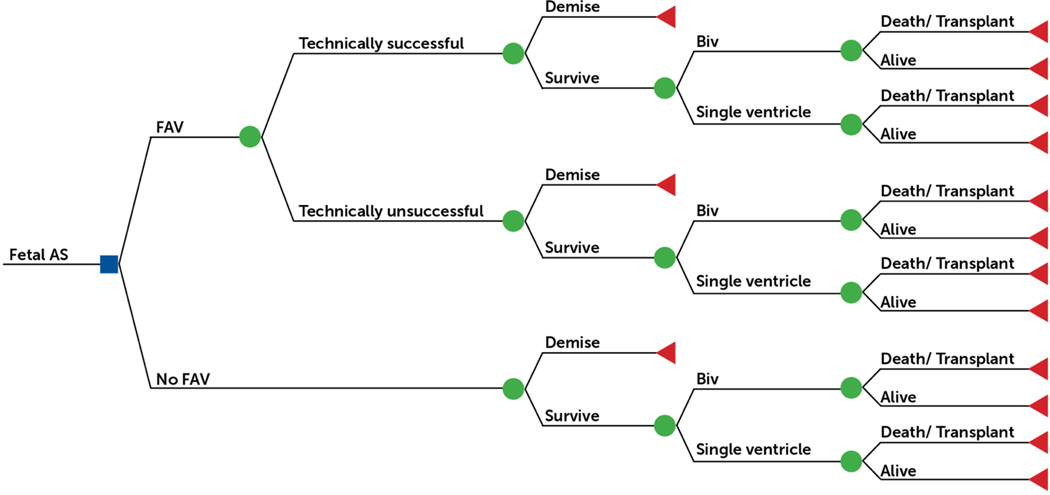
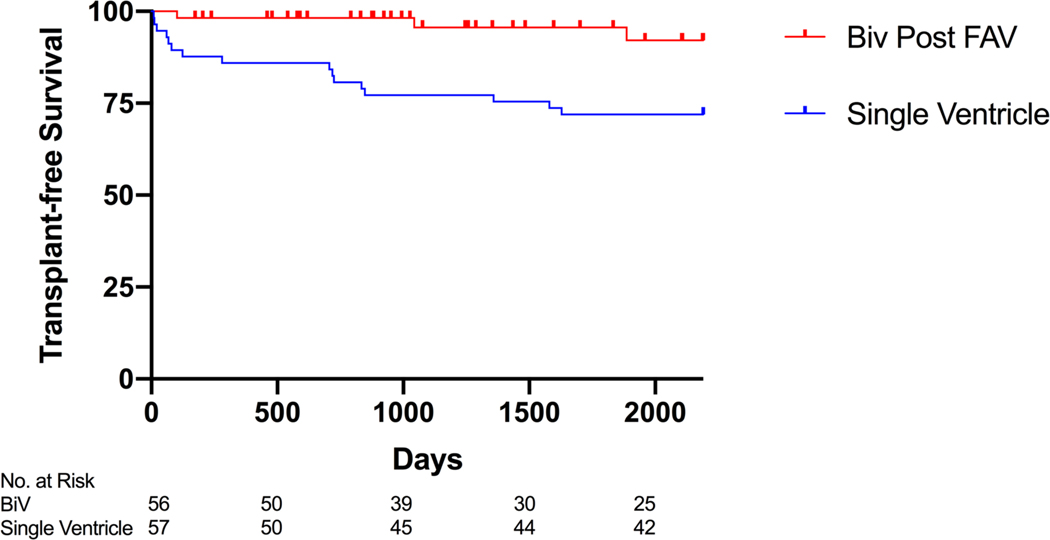
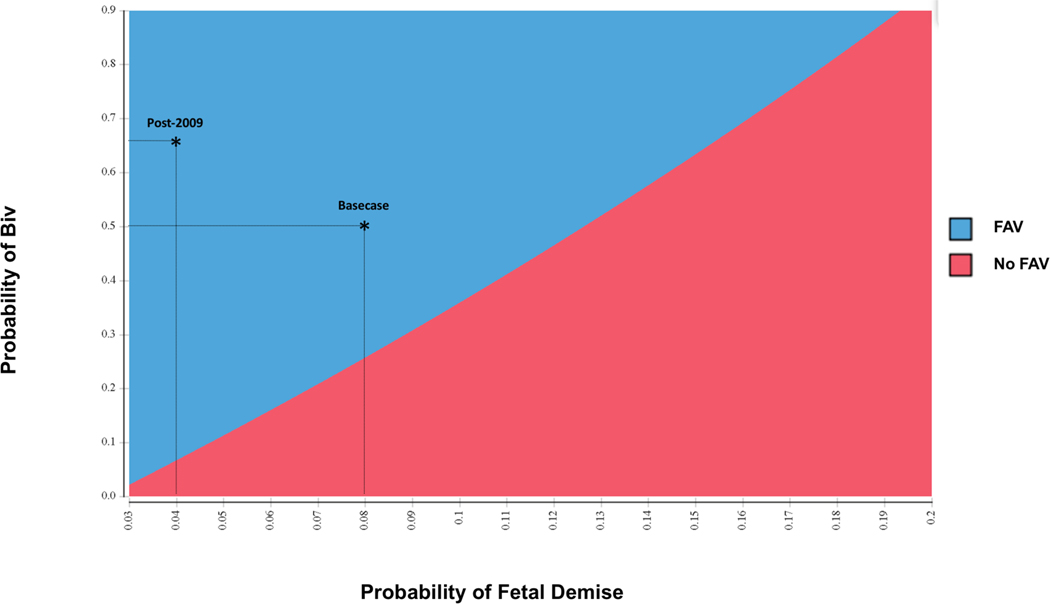
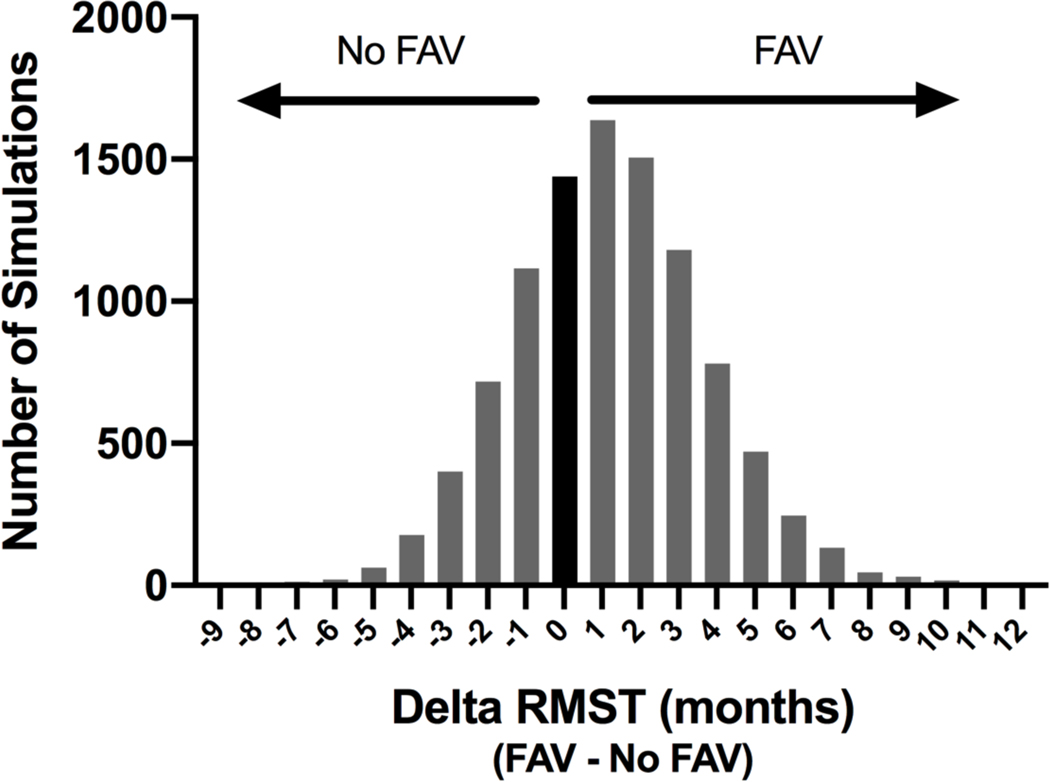
Methods and results: We performed a retrospective analysis of 143 fetuses who underwent FAV from 2000 to 2017 and a secondary analysis of the Pediatric Heart Network Single Ventricle Reconstruction trial. Using these results, we developed a decision model to estimate probability of transplant-free survival from fetal diagnosis to age 6 years and postnatal restricted mean transplant-free survival time. FAV was technically successful in 84% of 143 fetuses with fetal demise in 8%. Biventricular circulation was achieved in 50% of 111 live-born infants with successful FAV but in only 16% of the 19 patients with unsuccessful FAV. The model projected overlapping probabilities of transplant-free survival to age 6 years at 75% (95% CI, 67%-82%) with FAV versus 72% (95% CI, 61%-82%) with expectant fetal management, resulting in a restricted mean transplant-free survival time benefit of 1.2 months. When limiting analyses to the improved FAV experience since 2009 to reflect current practice, (probability of technical success [94%], fetal demise [4%], and biventricular circulation [66%]), the model projected that FAV increased the probability of survival to age 6 years to 82% (95% CI, 73%-89%). Expectant management is favored if risk of fetal demise exceeded 12% or probability of biventricular circulation fell below 26%, but FAV remained favored over plausible recent range of technical success.
Conclusions: Our model suggests that FAV provides a modest, medium-term survival benefit over expectant fetal management. Appropriate patient selection and low risk of fetal demise with FAV are critical factors for obtaining a survival benefit.
Keywords: fetal heart; hypoplastic left heart syndrome; infant; probability.
Figures
Comment in
-
Decisions, Decisions, Decisions…: A Novel Approach Helps Evaluate Potential Benefit of Fetal Aortic Valvuloplasty.Circ Cardiovasc Qual Outcomes. 2020 Apr;13(4):e006636. doi: 10.1161/CIRCOUTCOMES.120.006636. Epub 2020 Apr 7. Circ Cardiovasc Qual Outcomes. 2020. PMID: 32252550 No abstract available.
References
-
- Danford DA, Cronican P. Hypoplastic left heart syndrome: progression of left ventricular dilation and dysfunction to left ventricular hypoplasia in utero. Am Heart J. 1992;123:1712–1713. http://www.ncbi.nlm.nih.gov/pubmed/1595559. - PubMed
-
- Gardiner HM, Kovacevic A, Tulzer G, Sarkola T, Herberg U, Dangel J, Öhman A, Bartrons J, Carvalho JS, Jicinska H, Fesslova V, Averiss I, Mellander M, Fetal Working Group of the AEPC. Natural history of 107 cases of fetal aortic stenosis from a European multicenter retrospective study. Ultrasound Obstet Gynecol. 2016;48:373–381. doi: 10.1002/uog.15876 - DOI - PubMed
-
- Mäkikallio K, McElhinney DB, Levine JC, Marx GR, Colan SD, Marshall AC, Lock JE, Marcus EN, Tworetzky W. Fetal aortic valve stenosis and the evolution of hypoplastic left heart syndrome: patient selection for fetal intervention. Circulation. 2006;113:1401–1405. doi: 10.1161/CIRCULATIONAHA.105.588194 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
