

Efficacy and safety of concurrent chemoradiotherapy in ECOG 2 patients with locally advanced non-small-cell lung cancer: a subgroup analysis of a randomized phase III trial
- PMID: 32252680
- PMCID: PMC7137304
- DOI: 10.1186/s12885-020-06780-x
Efficacy and safety of concurrent chemoradiotherapy in ECOG 2 patients with locally advanced non-small-cell lung cancer: a subgroup analysis of a randomized phase III trial
Abstract
Background: There is no consensus on the therapeutic approach to ECOG 2 patients with locally advanced non-small-cell lung cancer (LA-NSCLC), despite the sizable percentage of these patients in clinical practice. This study focused on the efficacy, toxicity and the optimal chemotherapy regimen of CCRT in ECOG 2 patients in a phase III trial.
Methods: Patients capable of all self-care with bed rest for less than 50% of daytime were classified as ECOG 2 subgroup. A subgroup analysis was performed for ECOG 2 patients recruited in the phase III trial receiving concurrent EP (etoposide + cisplatin)/PC (paclitaxel + carboplatin) chemotherapy with intensity-modulated radiation therapy (IMRT) or three-dimensional conformal external beam radiation therapy (3D-CRT).
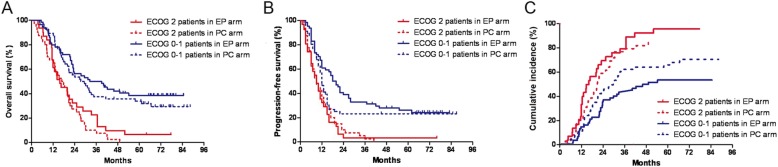
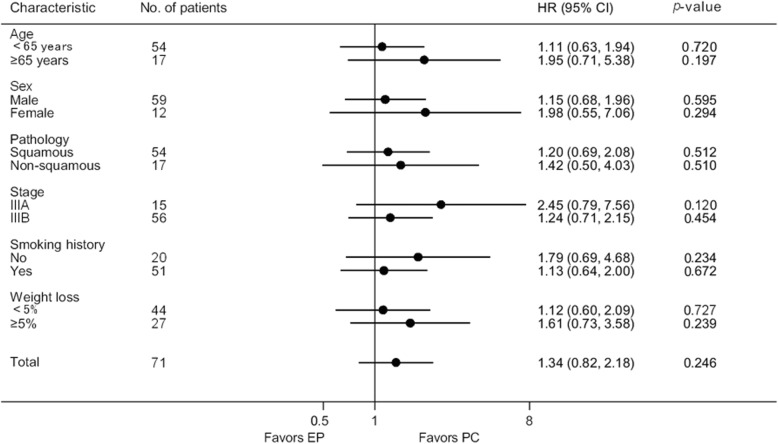
Results: A total of 71 ECOG 2 patients were enrolled into the study. Forty-six (64.8%) patients were treated with IMRT technique. The median overall survival (OS) and progression free survival (PFS) for ECOG 2 patients were 16.4 months and 9 months, respectively. No difference was observed in treatment compliance and toxicities between ECOG 2 patients and ECOG 0-1 patients. Within the ECOG 2 group (31 in the EP arm and 40 in the PC arm), median OS and 3-year OS were 15.7 months and 37.5% for the EP arm, and 16.8 months and 7.5% for the PC arm, respectively (p = 0.243). The incidence of grade ≥ 3 radiation pneumonitis was higher in the PC arm (17.5% vs. 0.0%, p = 0.014) with 5 radiation pneumonitis related deaths, while the incidence of grade 3 esophagitis was numerically higher in the EP arm (25.8% vs. 10.0%, p = 0.078).
Conclusions: CCRT provided ECOG 2 patients promising outcome with acceptable toxicities. EP might be superior to PC in terms of safety profile in the setting of CCRT for ECOG 2 patients. Prospective randomized studies based on IMRT technique are warranted to validate our findings.
Trial registration: ClinicalTrials.gov registration number: NCT01494558. (Registered 19 December 2011).
Keywords: Chemoradiotherapy; ECOG 2; Efficacy; Locally advanced; Non-small-cell lung cancer; Toxicity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Chansky K, Sculier JP, Crowley JJ, Giroux D, Van Meerbeeck J, Goldstraw P. The International Association for the Study of Lung Cancer staging project: prognostic factors and pathologic TNM stage in surgically managed non-small cell lung cancer. J Thoracic Oncology. 2009;4(7):792–801. doi: 10.1097/JTO.0b013e3181a7716e. - DOI - PubMed
-
- Auperin A, Le Pechoux C, Rolland E, Curran WJ, Furuse K, Fournel P, Belderbos J, Clamon G, Ulutin HC, Paulus R, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010;28(13):2181–2190. doi: 10.1200/JCO.2009.26.2543. - DOI - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
