

Expression of interferon-regulated genes in juvenile dermatomyositis versus Mendelian autoinflammatory interferonopathies
- PMID: 32252809
- PMCID: PMC7137415
- DOI: 10.1186/s13075-020-02160-9
Expression of interferon-regulated genes in juvenile dermatomyositis versus Mendelian autoinflammatory interferonopathies
Abstract
Background: Juvenile dermatomyositis (JDM) is a systemic autoimmune disease with a prominent interferon (IFN) signature, but the pathogenesis of JDM and the etiology of its IFN signature remain unknown. The Mendelian autoinflammatory interferonopathies, Chronic Atypical Neutrophilic Dermatosis with Lipodystrophy and Elevated temperature (CANDLE) and STING-Associated Vasculopathy with onset in Infancy (SAVI), are caused by genetic mutations and have extremely elevated IFN signatures thought to drive pathology. The phenotypic overlap of some clinical features of CANDLE and SAVI with JDM led to the comparison of a standardized interferon-regulated gene score (IRG-S) in JDM and myositis-specific autoantibody (MSA) JDM subgroups, with CANDLE and SAVI.
Methods: A peripheral 28-component IRG-S assessed by NanoString™ in 57 JDM patients subtyped by MSA was compared with IRG-S in healthy controls (HC) and CANDLE/SAVI patients. Principal component analysis (PCA) was performed, and individual genes were evaluated for their contribution to the score. IRG-S were correlated with disease assessments and patient characteristics.
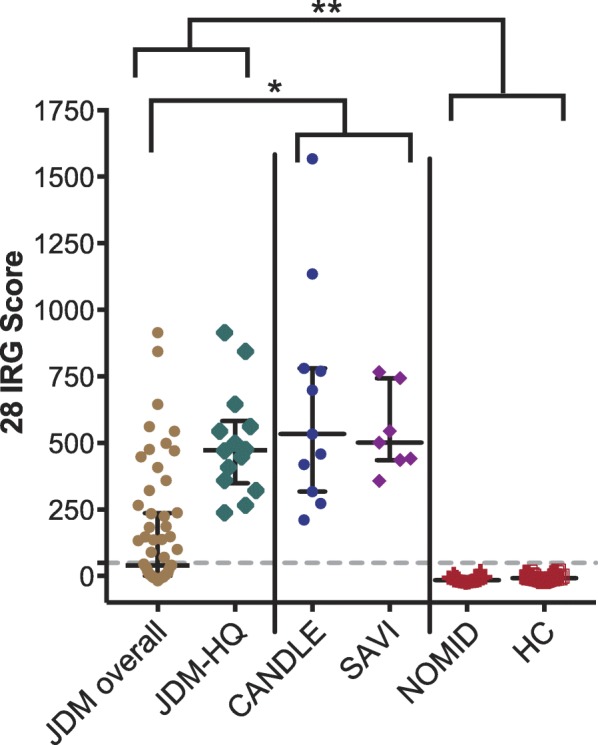
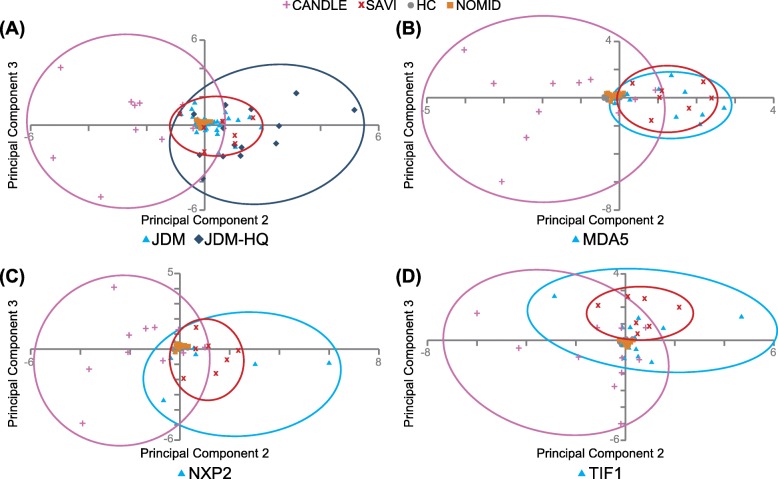
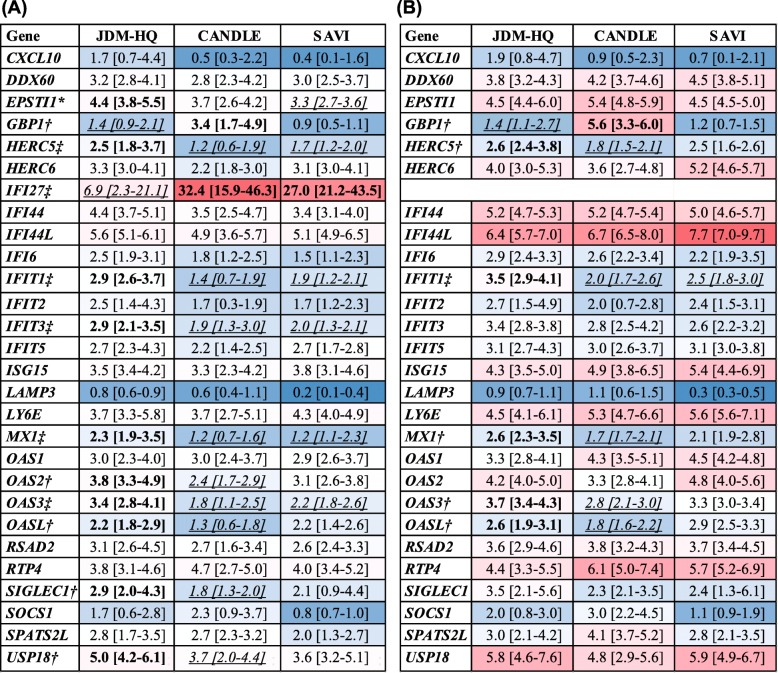
Results: IRG-S in JDM patients were significantly higher than in HC but lower than in CANDLE or SAVI. JDM IRG-S overlapped more with SAVI than CANDLE by PCA. Among MSA groups, anti-MDA5 autoantibody-positive patients' IRG-S overlapped most with SAVI. The IFI27 proportion was significantly higher in SAVI and CANDLE than JDM, but IFIT1 contributed more to IRG-S in JDM. Overall, the contribution of individual interferon-regulated genes (IRG) in JDM was more similar to SAVI. IRG-S correlated moderately with JDM disease activity measures (rs = 0.33-0.47) and more strongly with skin activity (rs = 0.58-0.79) in anti-TIF1 autoantibody-positive patients. Weakness and joint disease activity (multinomial OR 0.91 and 3.3) were the best predictors of high IRG-S.
Conclusions: Our findings demonstrate peripheral IRG expression in JDM overlaps with monogenic interferonopathies, particularly SAVI, and correlates with disease activity. Anti-MDA5 autoantibody-positive JDM IRG-S were notably more similar to SAVI. This may reflect both a shared IFN signature, which is driven by IFN-β and STING pathways in SAVI, as well as the shared phenotype of vasculopathy in SAVI and JDM, particularly in anti-MDA5 autoantibody-positive JDM, and indicate potential therapeutic targets for JDM.
Trial registration: ClinicalTrials.gov NCT02974595.
Keywords: (3–10): juvenile dermatomyositis; Biomarkers; Interferon; Interferonopathy; Myositis; Myositis-specific autoantibodies; Pediatric rheumatology.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Tansley SL, Simou S, Shaddick G, Betteridge ZE, Almeida B, Gunawardena H, Thomson W, Beresford MW, Midgley A, Muntoni F, et al. Autoantibodies in juvenile-onset myositis: their diagnostic value and associated clinical phenotype in a large UK cohort. J Autoimmun. 2017;84:55–64. doi: 10.1016/j.jaut.2017.06.007. - DOI - PMC - PubMed
-
- Habers GE, Huber AM, Mamyrova G, Targoff IN, O'Hanlon TP, Adams S, Pandey JP, Boonacker C, van Brussel M, Miller FW, et al. Brief report: association of myositis autoantibodies, clinical features, and environmental exposures at illness onset with disease course in juvenile myositis. Arthritis Rheumatol. 2016;68(3):761–768. doi: 10.1002/art.39466. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
