

Everolimus versus alpelisib in advanced hormone receptor-positive HER2-negative breast cancer: targeting different nodes of the PI3K/AKT/mTORC1 pathway with different clinical implications
- PMID: 32252811
- PMCID: PMC7137211
- DOI: 10.1186/s13058-020-01271-0
Everolimus versus alpelisib in advanced hormone receptor-positive HER2-negative breast cancer: targeting different nodes of the PI3K/AKT/mTORC1 pathway with different clinical implications
Abstract
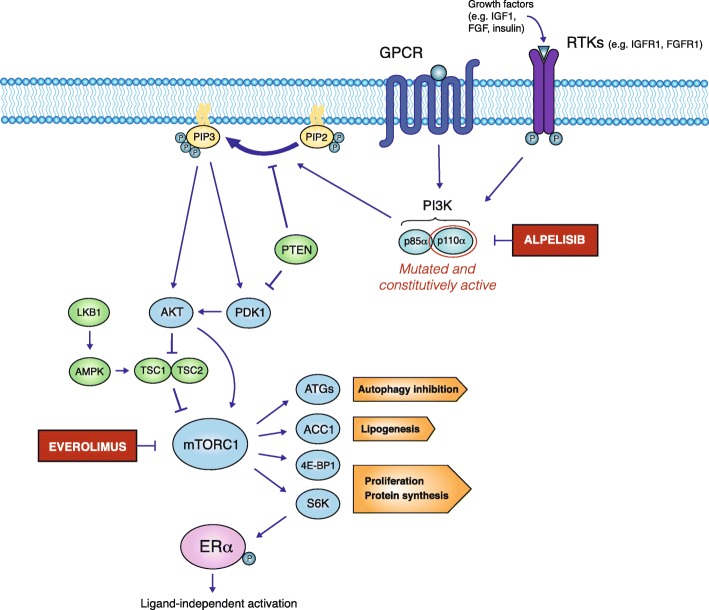
Background: The PI3K/AKT/mTORC1 axis is implicated in hormone receptor-positive HER2-negative metastatic breast cancer (HR+ HER2- mBC) resistance to anti-estrogen treatments. Based on results of the BOLERO-2 trial, the mTORC1 inhibitor everolimus in combination with the steroidal aromatase inhibitor (AI) exemestane has become a standard treatment for patients with HR+ HER2- mBC resistant to prior non-steroidal AI therapy. In the recent SOLAR-1 trial, the inhibitor of the PI3K alpha subunit (p110α) alpelisib in combination with fulvestrant prolonged progression-free survival (PFS) when compared to fulvestrant alone in patients with PIK3CA-mutated HR+ HER2- mBC that progressed after/on previous AI treatment. Therefore, two different molecules targeting the PI3K/AKT/mTORC1 axis, namely everolimus and alpelisib, are available for patients progressing on/after previous AI treatment, but it is unclear how to optimize their use in the clinical practice. Here, we reviewed the available clinical evidence deriving from the BOLERO-2 and SOLAR-1 trials to compare efficacy and safety profiles of everolimus and alpelisib in advanced HR+ HER2- BC treatment. Adding either compound to standard endocrine therapy provided similar absolute and relative PFS advantage. In the SOLAR-1 trial, a 76% incidence of grade (G) 3 or 4 (G3/G4) adverse events was reported, while G3/G4 toxicities occurred in 42% of patients in the BOLERO-2 trial. While alpelisib was only effective in patients with PIK3CA-mutated neoplasms, retrospective analyses indicate that everolimus improves exemestane efficacy independently of PIK3CA mutational status.
Conclusions: Based on the available efficacy and safety data, the "new" alpelisib may be burdened by higher incidence of severe adverse events, higher costs, and anticancer efficacy that is limited to PIK3CA-mutated tumors when compared to the "old" everolimus. Therefore, the everolimus-exemestane combination remains an effective and reasonably well-tolerated therapeutic option for HR+ HER2- mBC patients progressing after/on previous AI treatment, independently of PIK3CA mutational status.
Keywords: Advanced breast cancer; Alpelisib; Efficacy comparisons; Endocrine therapy; Everolimus; Hormone receptor-positive breast cancer; PI3K; PIK3CA mutations; mTORC1.
Conflict of interest statement
F.d.B. received personal fees from Novartis for expert presentations and as a member of the advisory board. No other disclosures were reported.
Figures
References
-
- Crowder RJ, Phommaly C, Tao Y, Hoog J, Luo J, Perou CM, Parker JS, Miller MA, Huntsman DG, Lin L, et al. PIK3CA and PIK3CB inhibition produce synthetic lethality when combined with estrogen deprivation in estrogen receptor-positive breast cancer. Cancer Res. 2009;69(9):3955–3962. doi: 10.1158/0008-5472.CAN-08-4450. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
