

Clinical efficacy and prognostic factors of CT-guided 125I brachytherapy for the palliative treatment of retroperitoneal metastatic lymph nodes
- PMID: 32252826
- PMCID: PMC7137200
- DOI: 10.1186/s40644-020-00299-x
Clinical efficacy and prognostic factors of CT-guided 125I brachytherapy for the palliative treatment of retroperitoneal metastatic lymph nodes
Abstract
Background: Due to the unique anatomical location of retroperitoneal metastatic lymph nodes, current treatment options are limited. This study was designed to explore the clinical efficacy and prognostic factors of CT-guided 125I brachytherapy for the treatment of retroperitoneal metastatic lymph nodes.
Methods: We retrospectively evaluated 92 patients received 125I brachytherapy for retroperitoneal metastatic lymph nodes. A layered Cox proportional hazards model was established to filter out the independent factors affecting local tumor progression-free survival (LTPFS).
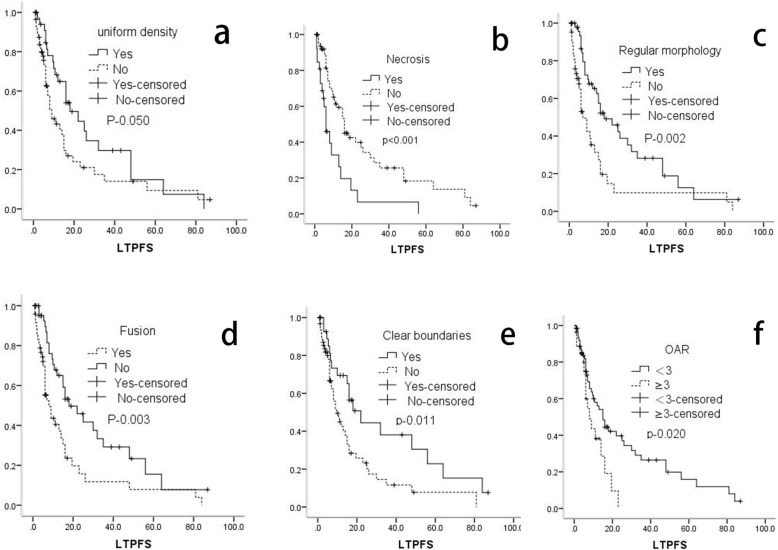
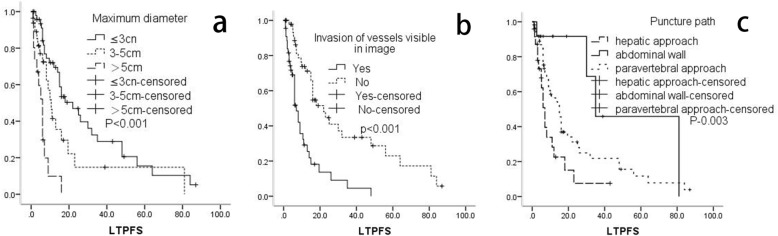
Results: The median LTPFS was 8 months. Metastatic lymph node with uniform density (p-0.009), clear boundaries (p-0.011), regular morphology (P < 0.001), and < 3 organs at risk of metastasis (p-0.020) were associated with better LTPFS. Necrotic lymph nodes (p < 0.001), fusion (p-0.003), and invasion of vessels visible on images (p < 0.001) were associated with poor LTPFS. Puncture path through abdominal wall or paravertebral approach were also associated with better LTPFS than a hepatic approach (P < 0.05). A maximum diameter ≤ 3 cm (P-0.031) or 3-5 cm (P-0.018) were also associated with significantly better LTPFS than a maximum diameter ≥ 5 cm. The Cox proportional hazards model suggested that lymph nodes invaded the large vessels visible on images, maximum diameter and puncture path were independent risk factors for LTPFS.
Conclusion: CT-guided 125I brachytherapy is an optional palliative treatment modality for retroperitoneal metastatic lymph nodes, which can provide high local control without severe complications. Better preoperative planning, intraoperative implementation, better choice of puncture path, and selection of appropriate tumor size are important factors that can improve the clinical efficacy of 125I brachytherapy for retroperitoneal metastatic lymph nodes.
Keywords: 125I brachytherapy; 125I seed; Retroperitoneal metastatic lymph nodes.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
