

Intravenous Iron Dosing and Infection Risk in Patients on Hemodialysis: A Prespecified Secondary Analysis of the PIVOTAL Trial
- PMID: 32253271
- PMCID: PMC7217408
- DOI: 10.1681/ASN.2019090972
Intravenous Iron Dosing and Infection Risk in Patients on Hemodialysis: A Prespecified Secondary Analysis of the PIVOTAL Trial
Abstract
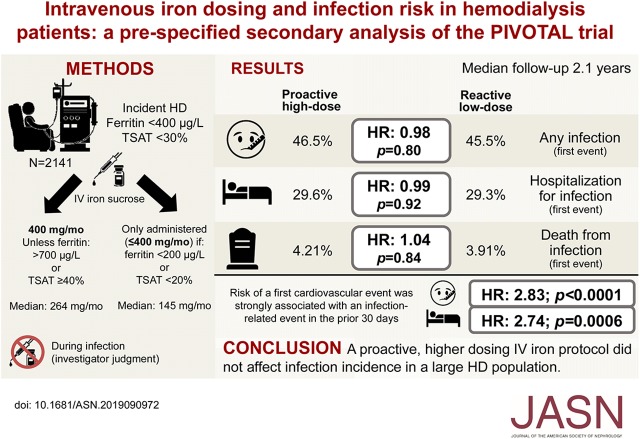
Background: Experimental and observational studies have raised concerns that giving intravenous (IV) iron to patients, such as individuals receiving maintenance hemodialysis, might increase the risk of infections. The Proactive IV Iron Therapy in Haemodialysis Patients (PIVOTAL) trial randomized 2141 patients undergoing maintenance hemodialysis for ESKD to a high-dose or a low-dose IV iron regimen, with a primary composite outcome of all-cause death, heart attack, stroke, or hospitalization for heart failure. Comparison of infection rates between the two groups was a prespecified secondary analysis.
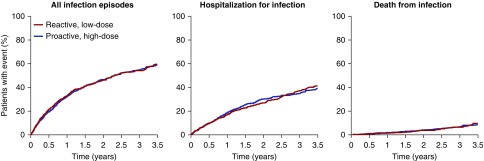
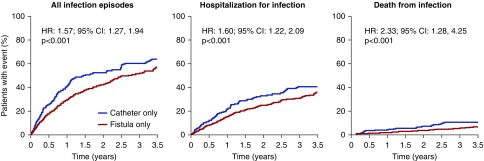
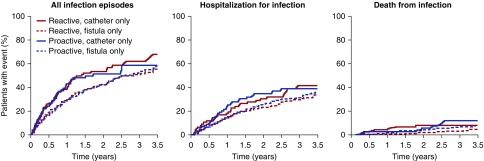
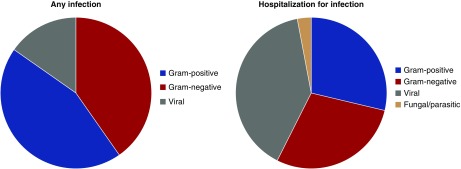
Methods: Secondary end points included any infection, hospitalization for infection, and death from infection; we calculated cumulative event rates for these end points. We also interrogated the interaction between iron dose and vascular access (fistula versus catheter).
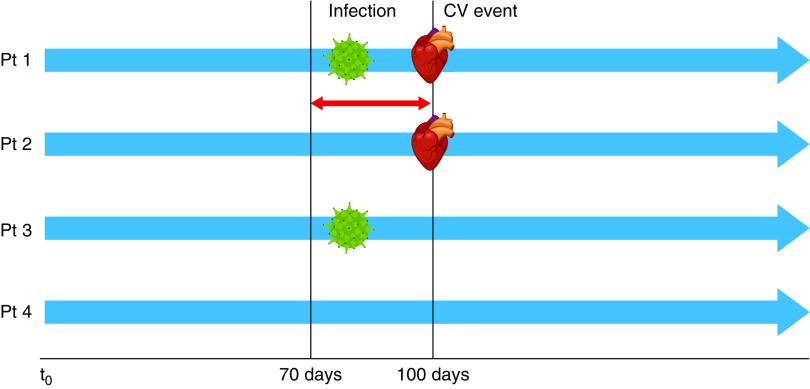
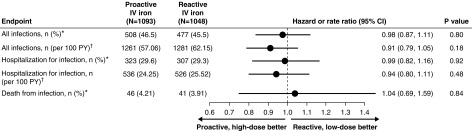
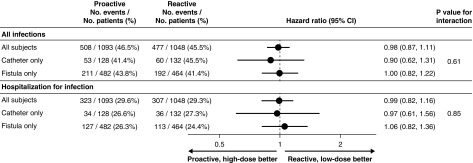
Results: We found no significant difference between the high-dose IV iron group compared with the lose-dose group in event rates for all infections (46.5% versus 45.5%, respectively, which represented incidences of 63.3 versus 69.4 per 100 patient years, respectively); rates of hospitalization for infection (29.6% versus 29.3%, respectively) also did not differ. We did find a significant association between risk of a first cardiovascular event and any infection in the previous 30 days. Compared with patients undergoing dialysis with an arteriovenous fistula, those doing so via a catheter had a higher incidence of having any infection, hospitalization for infection, or fatal infection, but IV iron dosing had no effect on these outcomes.
Conclusions: The high-dose and low-dose IV iron groups exhibited identical infection rates. Risk of a first cardiovascular event strongly associated with a recent infection.
Keywords: chronic kidney disease; hemodialysis; infections; intravenous iron; randomized controlled trial.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
The Value of Intravenous Iron: Beyond the Cave of Speculation.J Am Soc Nephrol. 2020 May;31(5):896-897. doi: 10.1681/ASN.2019121340. Epub 2020 Apr 6. J Am Soc Nephrol. 2020. PMID: 32253272 Free PMC article. No abstract available.
-
At the Crossroads for Intravenous Iron Dosing.J Am Soc Nephrol. 2020 Jul;31(7):1653-1654. doi: 10.1681/ASN.2020040540. Epub 2020 Jun 1. J Am Soc Nephrol. 2020. PMID: 32606032 Free PMC article. No abstract available.
-
Authors' Reply.J Am Soc Nephrol. 2020 Jul;31(7):1654. doi: 10.1681/ASN.2020050624. Epub 2020 Jun 1. J Am Soc Nephrol. 2020. PMID: 32606033 Free PMC article. No abstract available.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group: KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl 2: 279–335, 2012
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al.; ESC Scientific Document Group: 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 37: 2129–2200, 2016 - PubMed
-
- Macdougall IC, Bircher AJ, Eckardt KU, Obrador GT, Pollock CA, Stenvinkel P, et al.; Conference Participants: Iron management in chronic kidney disease: Conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int 89: 28–39, 2016 - PubMed
