

Serum uric acid level and subclinical left ventricular dysfunction: a community-based cohort study
- PMID: 32253826
- PMCID: PMC7261553
- DOI: 10.1002/ehf2.12691
Serum uric acid level and subclinical left ventricular dysfunction: a community-based cohort study
Abstract
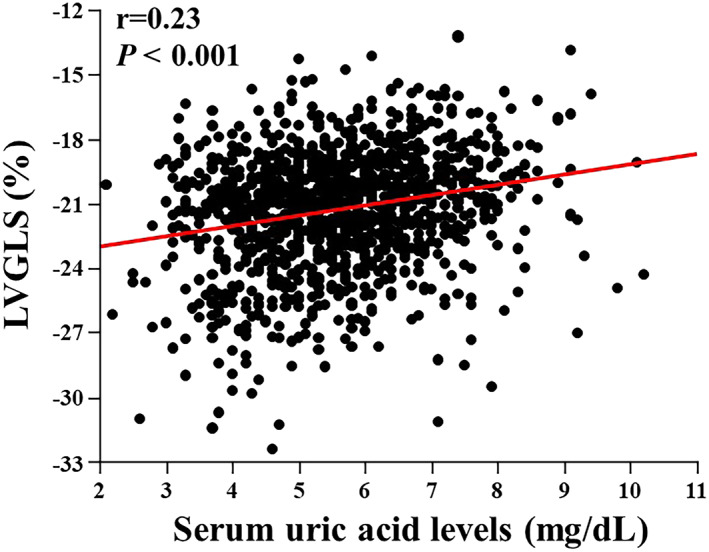
Aims: Although serum uric acid (SUA) level is correlated with oxidative stress and serves as a marker of poor prognosis in heart failure patients, its possible association with subclinical left ventricular (LV) dysfunction has not been evaluated. This study aimed to investigate the association between SUA and subclinical LV dysfunction in a sample of a general population without overt cardiac disease.
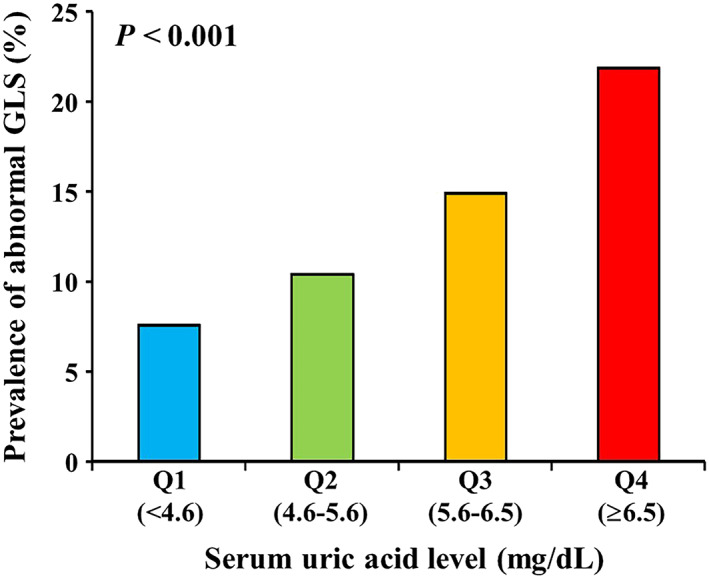
Methods and results: We examined 1175 participants who underwent extensive cardiovascular health check-up including laboratory tests and speckle-tracking echocardiography to assess LV global longitudinal strain (GLS). The association of SUA concentration, as a continuous variable and a categorical variable using quartiles, with the presence of abnormal LVGLS was assessed. Mean age was 62 ± 12 years, and 656 (56%) were male participants. Mean SUA was 5.6 ± 1.3 mg/dL (25th-75th percentile, 4.6-6.5 mg/dL). The prevalence of abnormal LVGLS (greater than -18.6%) was greatest in the upper quartile of SUA. In multivariable analysis, SUA as a continuous variable was significantly associated with abnormal LVGLS [adjusted odds ratio (OR), 1.26 per 1 mg/dL; P = 0.008] independent of traditional cardiovascular risk factors, pertinent laboratory parameters and echocardiographic measures, and medications. In the categorical analysis, the upper quartile of SUA was independently associated with abnormal LVGLS in a fully adjusted model (adjusted OR, 2.28 vs. lowest quartile; P = 0.020).
Conclusions: In a sample of the general population, an elevated SUA was independently associated with subclinical LV dysfunction. Assessment of LVGLS may add important prognostic information in individuals with elevated SUA, even in the absence of overt cardiac disease.
Keywords: Echocardiography; Global longitudinal strain; Primary prevention; Uric acid.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures

References
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Lutsey PL, Mackey JS, Matchar DB, Matsushita K, Mussolino ME, Nasir K, O'Flaherty M, Palaniappan LP, Pandey A, Pandey DK, Reeves MJ, Ritchey MD, Rodriguez CJ, Roth GA, Rosamond WD, Sampson UKA, Satou GM, Shah SH, Spartano NL, Tirschwell DL, Tsao CW, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, On behalf of the American Heart Association Council on Epidemiology , Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart Disease and Stroke Statistics‐2018 Update: A Report From the American Heart Association. Circulation 2018; 137: e67–e492. - PubMed
-
- Leyva F, Anker S, Swan JW, Godsland IF, Wingrove CS, Chua TP, Stevenson JC, Coats AJ. Serum uric acid as an index of impaired oxidative metabolism in chronic heart failure. Eur Heart J 1997; 18: 858–865. - PubMed
-
- Leyva F, Anker SD, Godsland IF, Teixeira M, Hellewell PG, Kox WJ, Poole‐Wilson PA, Coats AJ. Uric acid in chronic heart failure: a marker of chronic inflammation. Eur Heart J 1998; 19: 1814–1822. - PubMed
-
- Anker SD, Doehner W, Rauchhaus M, Sharma R, Francis D, Knosalla C, Davos CH, Cicoira M, Shamim W, Kemp M, Segal R, Osterziel KJ, Leyva F, Hetzer R, Ponikowski P, Coats AJ. Uric acid and survival in chronic heart failure: validation and application in metabolic, functional, and hemodynamic staging. Circulation 2003; 107: 1991–1997. - PubMed
-
- Pascual‐Figal DA, Hurtado‐Martinez JA, Redondo B, Antolinos MJ, Ruiperez JA, Valdes M. Hyperuricaemia and long‐term outcome after hospital discharge in acute heart failure patients. Eur J Heart Fail 2007; 9: 518–524. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
