

Diminished responses to bodily threat and blunted interoception in suicide attempters
- PMID: 32254020
- PMCID: PMC7138608
- DOI: 10.7554/eLife.51593
Diminished responses to bodily threat and blunted interoception in suicide attempters
Abstract
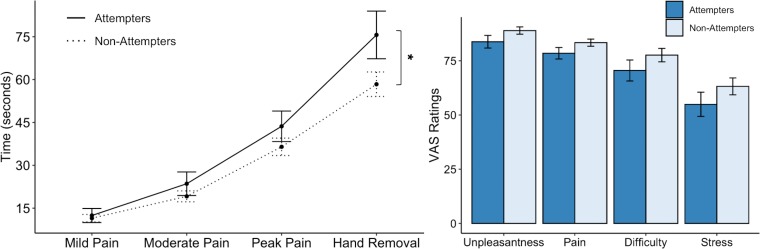
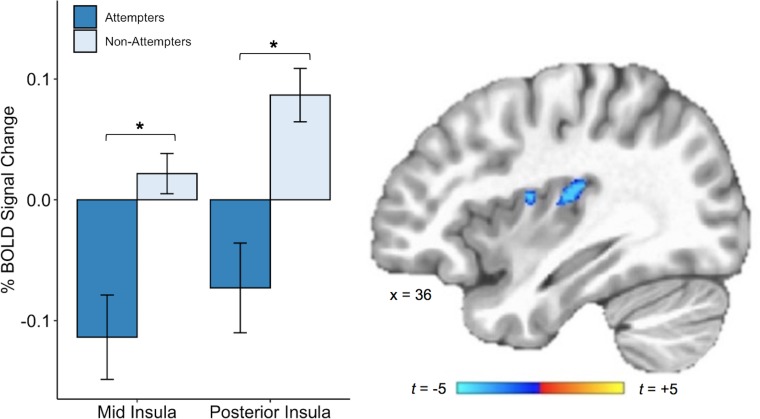
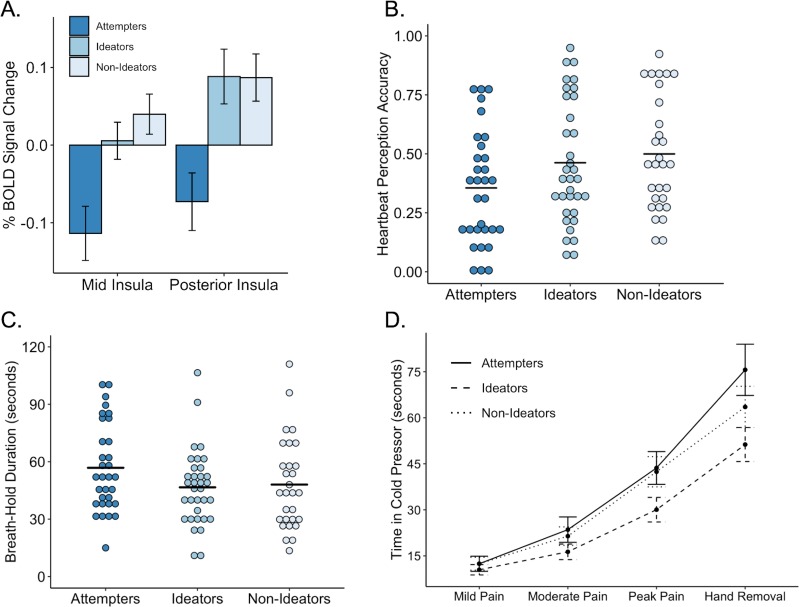
Psychological theories of suicide suggest that certain traits may reduce aversion to physical threat and increase the probability of transitioning from suicidal ideation to action. Here, we investigated whether blunted sensitivity to bodily signals is associated with suicidal action by comparing individuals with a history of attempted suicide to a matched psychiatric reference sample without suicide attempts. We examined interoceptive processing across a panel of tasks: breath-hold challenge, cold-pressor challenge, and heartbeat perception during and outside of functional magnetic resonance imaging. Suicide attempters tolerated the breath-hold and cold-pressor challenges for significantly longer and displayed lower heartbeat perception accuracy than non-attempters. These differences were mirrored by reduced activation of the mid/posterior insula during attention to heartbeat sensations. Our findings suggest that suicide attempters exhibit an 'interoceptive numbing' characterized by increased tolerance for aversive sensations and decreased awareness of non-aversive sensations. We conclude that blunted interoception may be implicated in suicidal behavior.
Keywords: fMRI; human; insula; interoception; neuroscience; pain; respiration; suicide.
Plain language summary
The human brain closely monitors body signals essential for our survival, including our heartbeat, our breathing and even the temperature of our skin. This mostly unconscious process is called interoception. It helps people perceive potential or actual threats and helps them to respond appropriately. For example, a person charged by a wild animal will act instinctively to run, fight or freeze. Unlike most creatures, humans show an ability to counteract these survival instincts, and are capable of intentionally engaging in behaviors that result in physical harm. Recent increases in the rate of suicide have made it more urgent to try to understand what leads to this behavior in humans. Now, DeVille et al. show that people with psychiatric disorders who have survived a suicide attempt have blunted interoception. In four experiments, people with a history of suicide attempts were compared to another group of individuals without a history of suicide attempts. The groups were carefully matched such that there were no significant differences in the demographic and clinical characteristics of the two groups, including in terms of their age, sex, body mass index and psychiatric symptoms. Both groups completed uncomfortable tasks like holding their breath or keeping their hand in icy cold water. The participants also completed two tasks that required them to focus on their own heartbeat, one of which was paired with functional magnetic resonance imaging. Those with a history of suicide attempts held their breath and kept their hand in cold water for longer, and also were less in tune with their heart rate. This “interoceptive numbing” was associated with less activity in part of the brain called the insular cortex. These differences could not be explained by the individuals having a psychiatric disorder or a history of considering suicide, or by them taking psychiatric medications. Instead, the interoceptive numbing was most often seen in individuals who made an attempt on their own life. The experiments identify physical characteristics that may differentiate people who attempt suicide from those who do not. This lays the groundwork for future research aimed at identifying biological indicators of suicide risk. More studies are needed to verify the results. If the results are verified, the next step would be prospective studies to determine whether measuring interoception can help clinicians predict who is at risk of a suicide attempt. If it does, it might give clinicians a new tool to try to prevent suicide by ensuring those at greatest risk receive appropriate care.
© 2020, DeVille et al.
Conflict of interest statement
DD, RK, JS, MP, SK No competing interests declared
Figures




References
-
- Aguilar EJ, García-Martí G, Martí-Bonmatí L, Lull JJ, Moratal D, Escartí MJ, Robles M, González JC, Guillamón MI, Sanjuán J. Left orbitofrontal and superior temporal gyrus structural changes associated to suicidal behavior in patients with schizophrenia. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2008;32:1673–1676. doi: 10.1016/j.pnpbp.2008.06.016. - DOI - PubMed
-
- Aupperle RL, Paulus MP, Kuplicki R, Touthang J, Victor T, Yeh HW, Khalsa SS, Tulsa 1000 Investigators Web-Based graphic representation of the life course of mental health: cross-sectional study across the spectrum of mood, anxiety, eating, and Substance use disorders. JMIR Mental Health. 2020;7:e16919. doi: 10.2196/16919. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
