

Determinants of loss to follow-up among HIV positive patients receiving antiretroviral therapy in a test and treat setting: A retrospective cohort study in Masaka, Uganda
- PMID: 32255796
- PMCID: PMC7138304
- DOI: 10.1371/journal.pone.0217606
Determinants of loss to follow-up among HIV positive patients receiving antiretroviral therapy in a test and treat setting: A retrospective cohort study in Masaka, Uganda
Abstract
Background: Retaining patients starting antiretroviral therapy (ART) and ensuring good adherence remain cornerstone of long-term viral suppression. In this era of test and treat (T&T) policy, ensuring that patients starting ART remain connected to HIV clinics is key to achieve the UNAIDS 90-90-90 targets. Currently, limited studies have evaluated the effect of early ART initiation on loss to follow up in a routine health care delivery setting. We studied the cumulative incidence, incidence rate of loss to follow up (LTFU), and factors associated with LTFU in a primary healthcare clinic that has practiced T&T since 2012.
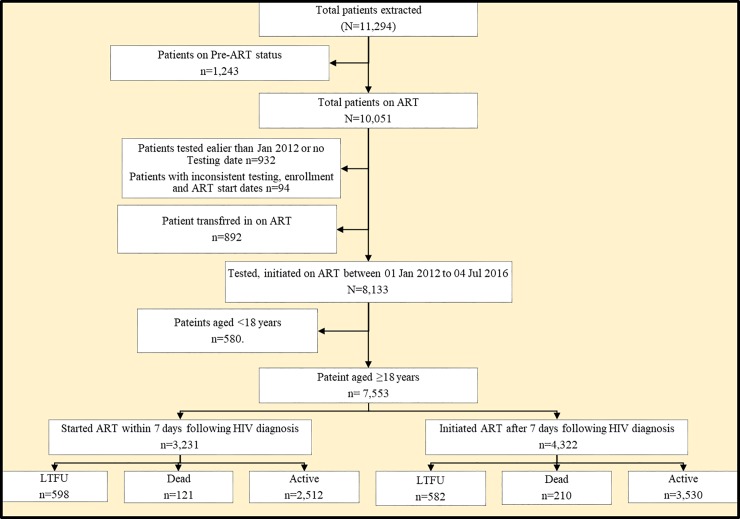
Methods: We retrospectively analyzed extracted routine program data on patients who started ART from January 2012 to 4th July 2016. We defined LTFU as failure of a patient to return to the HIV clinic for at least 90 days from the date of their last appointment. We calculated cumulative incidence, incidence rate and fitted a multivariable Cox proportion hazards regression model to determine factors associated with LTFU.
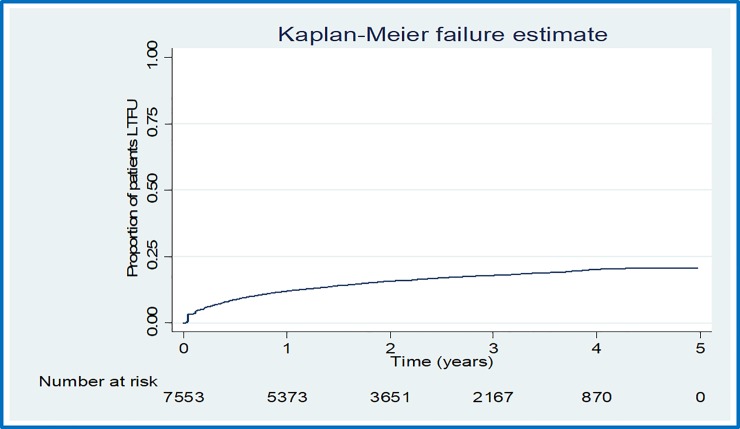
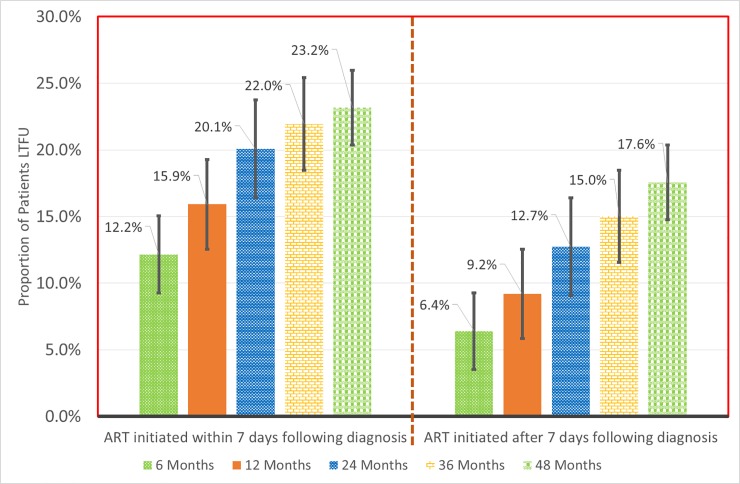
Results: Of the 7,553 patients included in our sample, 3,231 (42.8%) started ART within seven days following HIV diagnosis. There were 1,180 cases of LTFU observed over 15,807.7 person years at risk. The overall incidence rate (IR) of LTFU was 7.5 (95% CI, 7.1-7.9) per 100 person years of observation (pyo). Cumulative incidence of LTFU increased with duration of follow up from 8.9% (95% CI, 8.2-9.6%) at 6 months to 20.2% (95% CI, 19.0-21.4%) at 48 months. Predictors of elevated risk of LTFU were: starting ART within 7 days following HIV diagnosis ((aHR) = 1.69, 95% CI, 1.50-1.91), lack of a telephone set (aHR = 1.52, 95% CI, 1.35-1.71), CD4 cell count of 200-350μ/ml (aHR = 1.21, 95% CI, 1.01-1.45) and baseline WHO clinical stage 3 or 4 (aHR = 1.35, 95% CI, 1.10-1.65). Factors associated with a reduced risk of LTFU were: baseline age ≥25 years (aHR ranging from 0.62, 95% CI, 0.47-0.81 for age group 25-29 years to 0.24, 95% CI, 0.13-0.44 for age group ≥50 years), at least primary education level (aHR ranging from aHR = 0.77, 95% CI, 0.62-0.94 for primary education level to 0.50, 95% CI, 0.34-0.75 for post-secondary education level), and having a BMI ≥ 30 (aHR = 0.28, 95% CI, 0.15-0.51).
Conclusion: The risk of loss to follow up increased with time and was higher among patients who started ART within seven days following HIV diagnosis, higher among patients without a telephone set, lower among patients aged ≥ 25 years, lower among patients with at least primary education and lower among patients with BMI of ≥ 30. In this era of T&T, it will be important for HIV programs to initiate and continue enhanced therapeutic education programs that target high risk groups, as well as leveraging on mHealth to improve patients' retention on ART throughout the cascade of care.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organisation. 2017 WHO Data and Statistics. HIVAIDS Data Stat. 2018 [cited 2019 Feb 21]. Available from: https://www.who.int/hiv/data/en/
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. UNAIDS; 2014 Oct. http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf
-
- Grinsztejn B, Hosseinipour MC, Ribaudo HJ, Swindells S, Eron J, Chen YQ, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis. 2014;14:281–90. 10.1016/S1473-3099(13)70692-3 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
