

Limb salvage reconstruction: Radiologic features of common reconstructive techniques and their complications
- PMID: 32256002
- PMCID: PMC7125314
- DOI: 10.1016/j.jor.2020.03.043
Limb salvage reconstruction: Radiologic features of common reconstructive techniques and their complications
Abstract
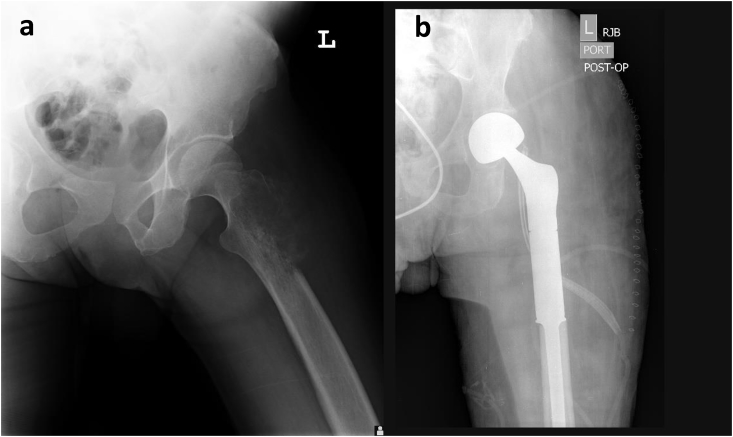
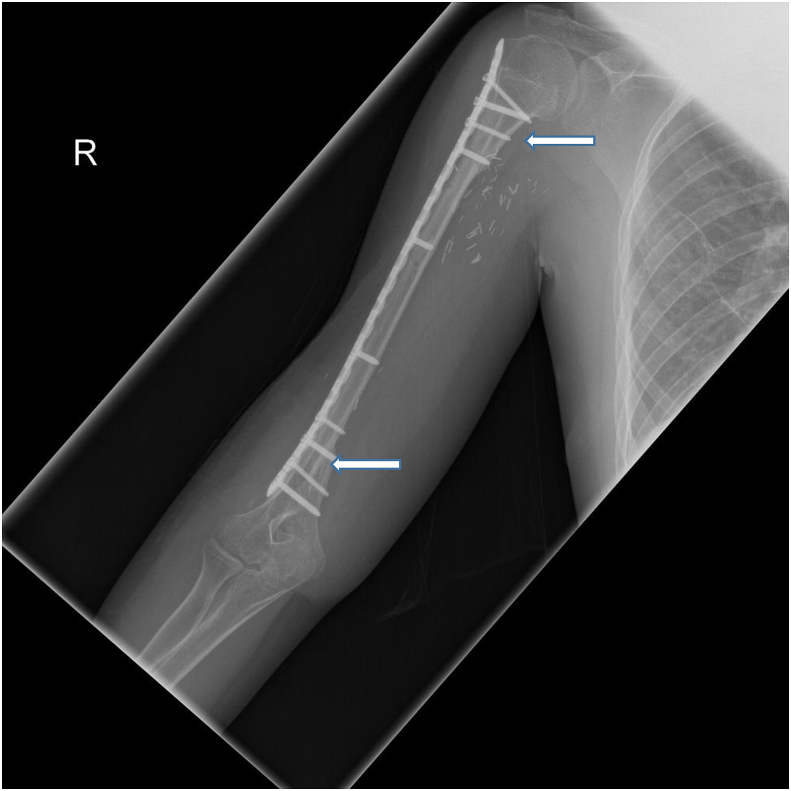
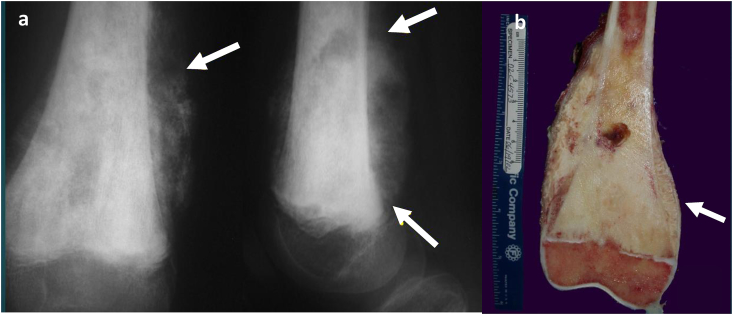
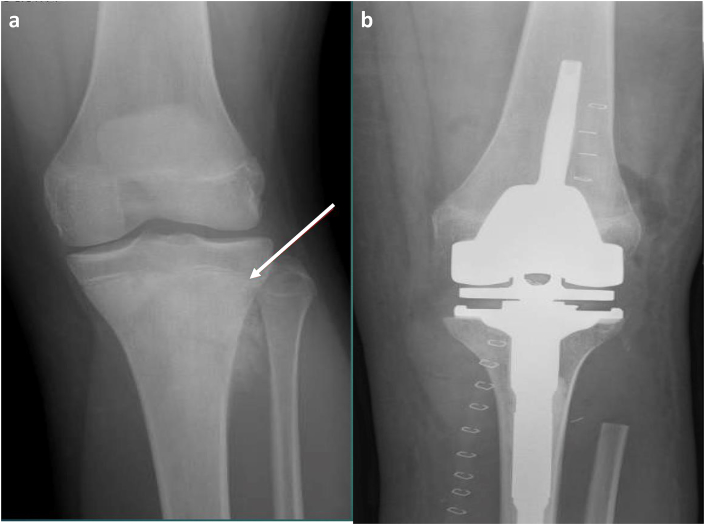
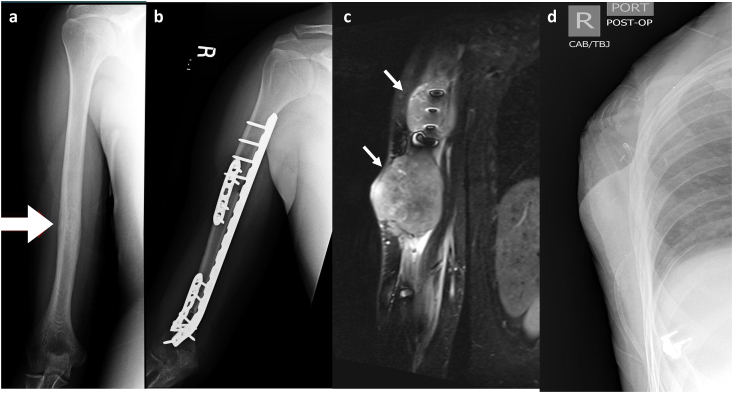
Limb salvage surgery refers to orthopaedic procedures designed to resect tumors and reconstruct limbs. Improvements in managing malignant bone lesions have led to a dramatic shift in limb salvage procedures. Orthopaedic surgeons now employ four main reconstructive procedures: endoprosthesis, autograft, bulk allograft, and allograft prosthetic composite. While each approach has its advantages, each technique is associated with complications. Furthermore, knowledge of procedure specific imaging findings can lead to earlier complication diagnosis and improved clinical outcomes. The aim of this article is to review leading reconstructive options available for limb salvage surgery and present a case series illustrating the associated complications.
Keywords: Allograft; Autograft; Endoprosthesis; Limb salvage.
© 2020 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
All authors declare that they have no conflict of interest. This article does not contain any studies with human participants or animals performed by any of the authors.
Figures

References
-
- DiCaprio M.R., Friedlaender G.E. Malignant bone tumors: limb sparing versus amputation. J Am Acad Orthop Surg. 2003;11(1):25–37. - PubMed
-
- Solooki S., Mostafavizadeh Ardestani S.M., Mahdaviazad H., Kardeh B. Function and quality of life among primary osteosarcoma survivors in Iran: amputation versus limb salvage. Musculoskelet Surg. 2017 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
