

A Short Series of Laparoscopic Mesenteric Bypasses for Chronic Mesenteric Ischemia
- PMID: 32256075
- PMCID: PMC7098165
- DOI: 10.2147/VHRM.S243264
A Short Series of Laparoscopic Mesenteric Bypasses for Chronic Mesenteric Ischemia
Abstract
Background: Laparoscopic aortomesenteric bypass may be performed to treat the chronic mesenteric ischemia patients who are not suitable for endovascular treatment. This study presents an initial experience with a limited series of laparoscopic mesenteric artery revascularization for the treatment of mesenteric ischemia.
Methods: Chronic mesenteric ischemia (CMI) patients with previous unsuccessful endovascular treatment or with arterial occlusion and extensive calcification precluding safe endovascular treatment were offered laparoscopic mesenteric revascularization. From October 2015 until November 2018, nine patients with CMI underwent laparoscopic revascularization. In addition to demographic data and perioperative results of the treatment, graft patency was assessed with Duplex ultrasound at 1, 3, 6 and 12 months, and annually thereafter. A descriptive analysis of the data was performed.
Results: All bypasses were constructed with an 8 mm ring enforced expanded polytetrafluoroethylene graft in a retrograde fashion (from infrarenal aorta or iliac artery) to either superior mesenteric artery or splenic artery (2 cases). Median operation time was 356 mins (range 247-492 mins). Five patients had a history of unsuccessful endovascular treatment. Laparoscopic technical success was 78%, and the primary open conversion rate was 22%. All laparoscopic revascularization procedures remained patent after discharge during a median follow-up time of 26 months (range 18-49 months). The primary graft patency at 30 days was 78%. Primary assisted, and secondary graft patency was 78% and 100%, respectively. Median weight gain was 2 kg (range 2-18 kg), and all patients achieved relief from postprandial pain and nausea. No mortality was observed during the follow-up period.
Conclusion: Laparoscopic aortomesenteric revascularization procedures for chronic mesenteric ischemia are feasible but require careful patient selection. These procedures should only be performed at referral centers by vascular surgeons with prior experience in laparoscopic vascular surgery.
Keywords: bypass; chronic mesenteric ischemia; intestinal ischemia; laparoscopy; mesenteric ischemia.
© 2020 Kazmi et al.
Conflict of interest statement
The authors have nothing to disclose.
Figures
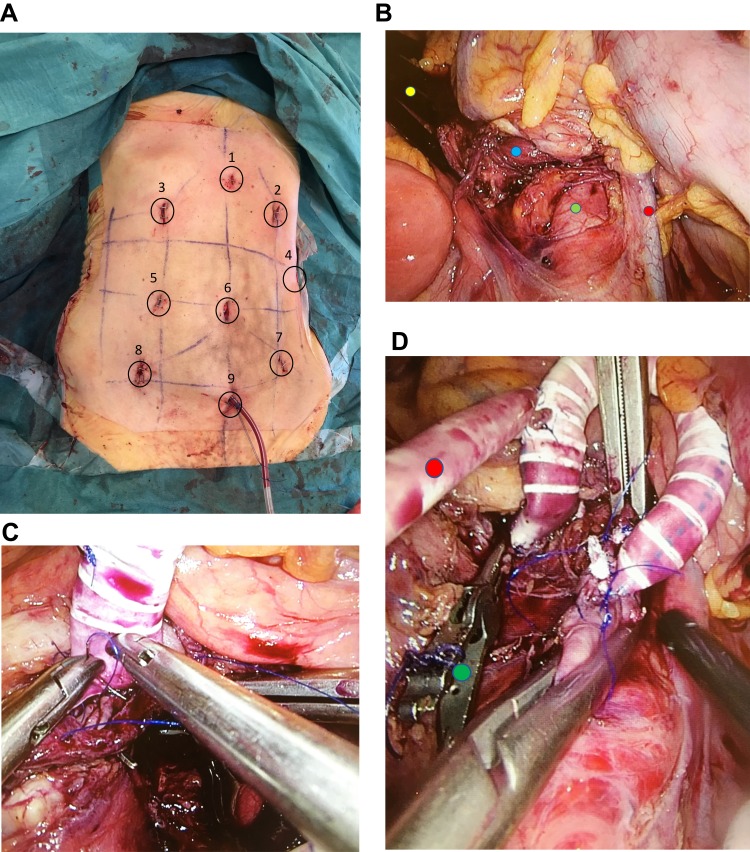
 ) and infrarenal aorta (
) and infrarenal aorta ( ). Treitz ligament is divided, and duodenum mobilized distally and held under a retractor (
). Treitz ligament is divided, and duodenum mobilized distally and held under a retractor ( ). Inferior mesenteric vein (
). Inferior mesenteric vein ( ). (C): End-to-side anastomosis with superior mesenteric artery. (D): Completed anastomoses on superior mesenteric artery and infrarenal abdominal aorta. Ring enforced expanded polytetrafluoroethylene graft with an end-to-side anastomosed 6 mm graft. Side graft (
). (C): End-to-side anastomosis with superior mesenteric artery. (D): Completed anastomoses on superior mesenteric artery and infrarenal abdominal aorta. Ring enforced expanded polytetrafluoroethylene graft with an end-to-side anastomosed 6 mm graft. Side graft ( ) is being flushed with heparinized NaCl to check the patency of anastomoses before the aortic and superior mesenteric artery clamps are removed. Laparoscopic bulldog artery clamp (
) is being flushed with heparinized NaCl to check the patency of anastomoses before the aortic and superior mesenteric artery clamps are removed. Laparoscopic bulldog artery clamp ( ).
).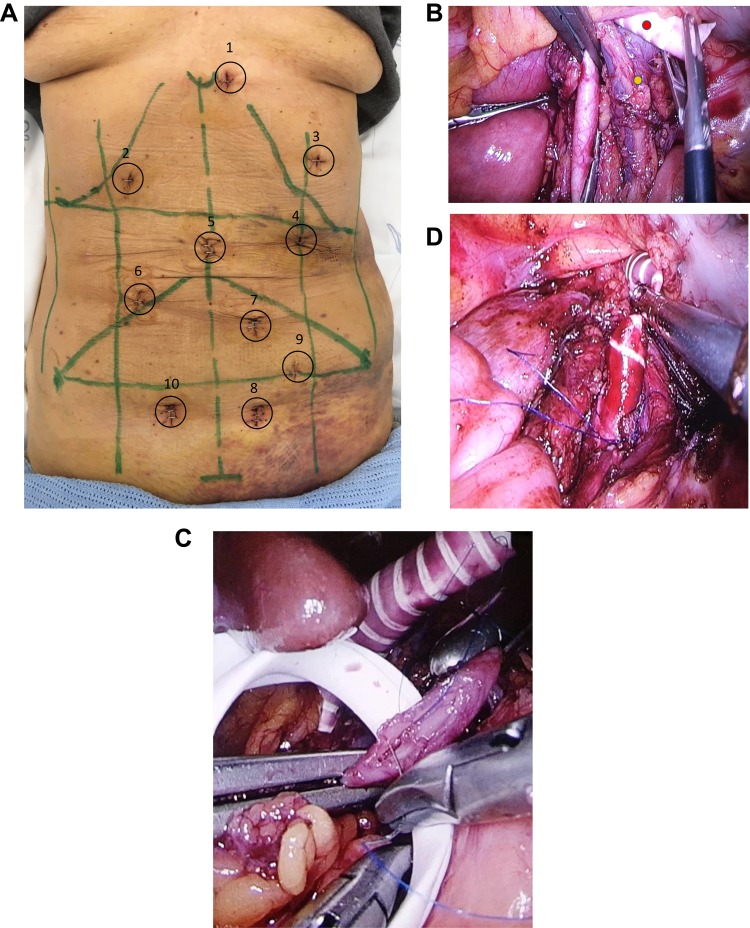
 ). Cross-clamped infrarenal aorta and left gonadal vein (
). Cross-clamped infrarenal aorta and left gonadal vein ( ). (C): Ring enforced expanded polytetrafluoroethylene graft is bein anastomosed end-to-side to a clamped splenic artery. Nathanson’s liver retractor is elevating the left liver lobe. (D): Completed end-to-side anastomosis to the infrarenal aorta.
). (C): Ring enforced expanded polytetrafluoroethylene graft is bein anastomosed end-to-side to a clamped splenic artery. Nathanson’s liver retractor is elevating the left liver lobe. (D): Completed end-to-side anastomosis to the infrarenal aorta.
Similar articles
-
Direct Retrograde Bypass is Preferable to Antegrade Bypass for Open Mesenteric Revascularization.Ann Vasc Surg. 2020 Jul;66:263-271. doi: 10.1016/j.avsg.2020.01.019. Epub 2020 Jan 10. Ann Vasc Surg. 2020. PMID: 31931133
-
Outcomes of antegrade and retrograde open mesenteric bypass for acute mesenteric ischemia.J Vasc Surg. 2019 Jan;69(1):129-140. doi: 10.1016/j.jvs.2018.04.063. Epub 2018 Jun 29. J Vasc Surg. 2019. PMID: 30580778
-
Durability of antegrade synthetic aortomesenteric bypass for chronic mesenteric ischemia.J Vasc Surg. 2002 Jun;35(6):1078-84. doi: 10.1067/mva.2002.124377. J Vasc Surg. 2002. PMID: 12042717
-
Mesenteric artery bypass: objective patency determination.J Vasc Surg. 1995 May;21(5):729-40; discussion 740-1. doi: 10.1016/s0741-5214(05)80004-7. J Vasc Surg. 1995. PMID: 7769732 Review.
-
Chronic mesenteric ischemia: Diagnosis and management.Prog Cardiovasc Dis. 2021 Mar-Apr;65:71-75. doi: 10.1016/j.pcad.2021.03.002. Epub 2021 Apr 24. Prog Cardiovasc Dis. 2021. PMID: 33901516 Review.
Cited by
-
A Review on Aorta Mesenteric Bypass in Surgical Management of Mesenteric Ischemia: Indications, Techniques and Outcomes.Maedica (Bucur). 2020 Sep;15(3):381-390. doi: 10.26574/maedica.2020.15.3.381. Maedica (Bucur). 2020. PMID: 33312256 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
