

Platelet-Inspired Nanocells for Targeted Heart Repair After Ischemia/Reperfusion Injury
- PMID: 32256277
- PMCID: PMC7111457
- DOI: 10.1002/adfm.201803567
Platelet-Inspired Nanocells for Targeted Heart Repair After Ischemia/Reperfusion Injury
Abstract
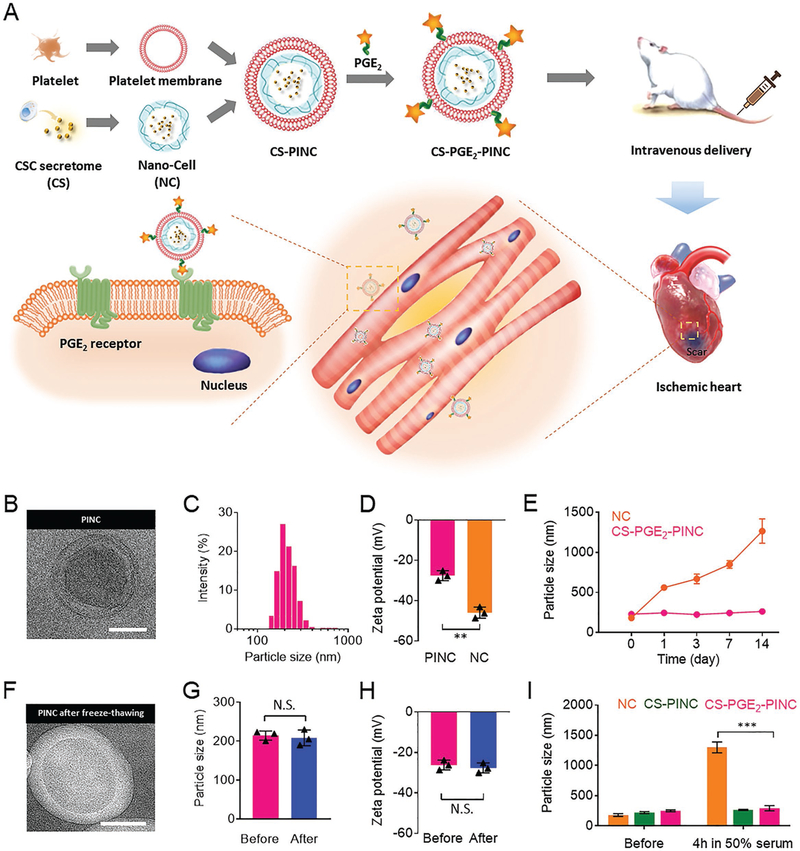
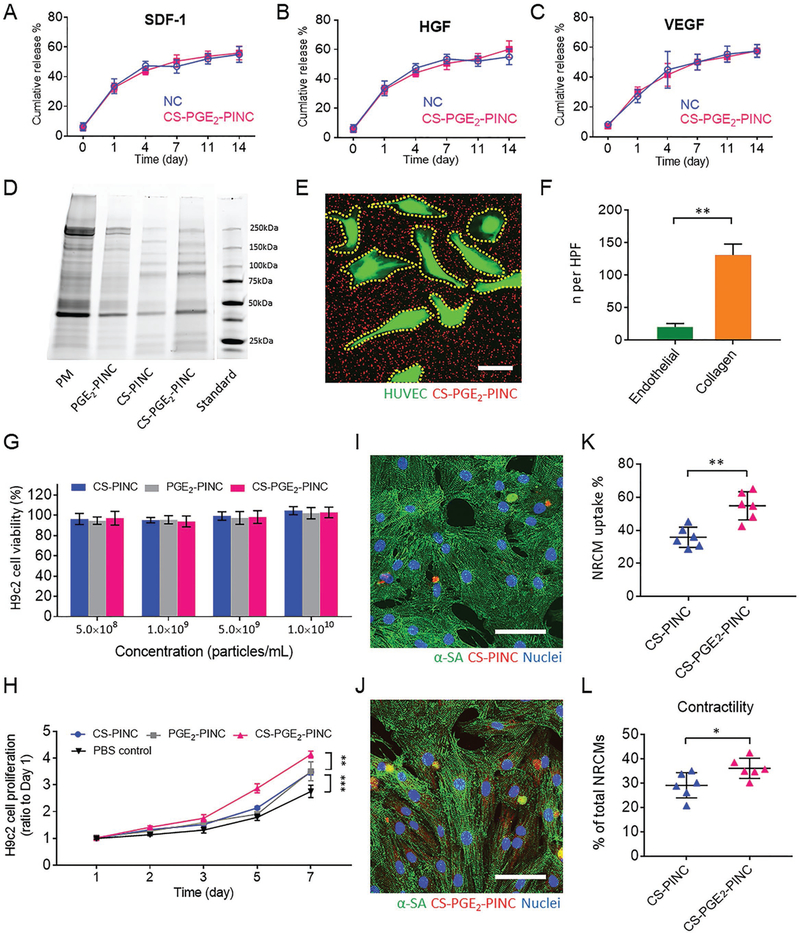
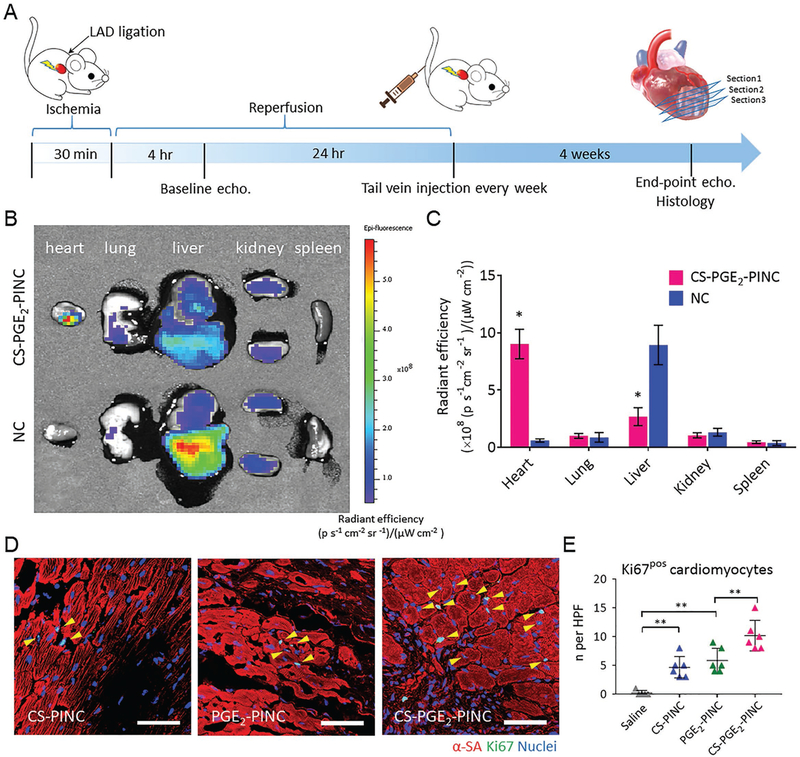
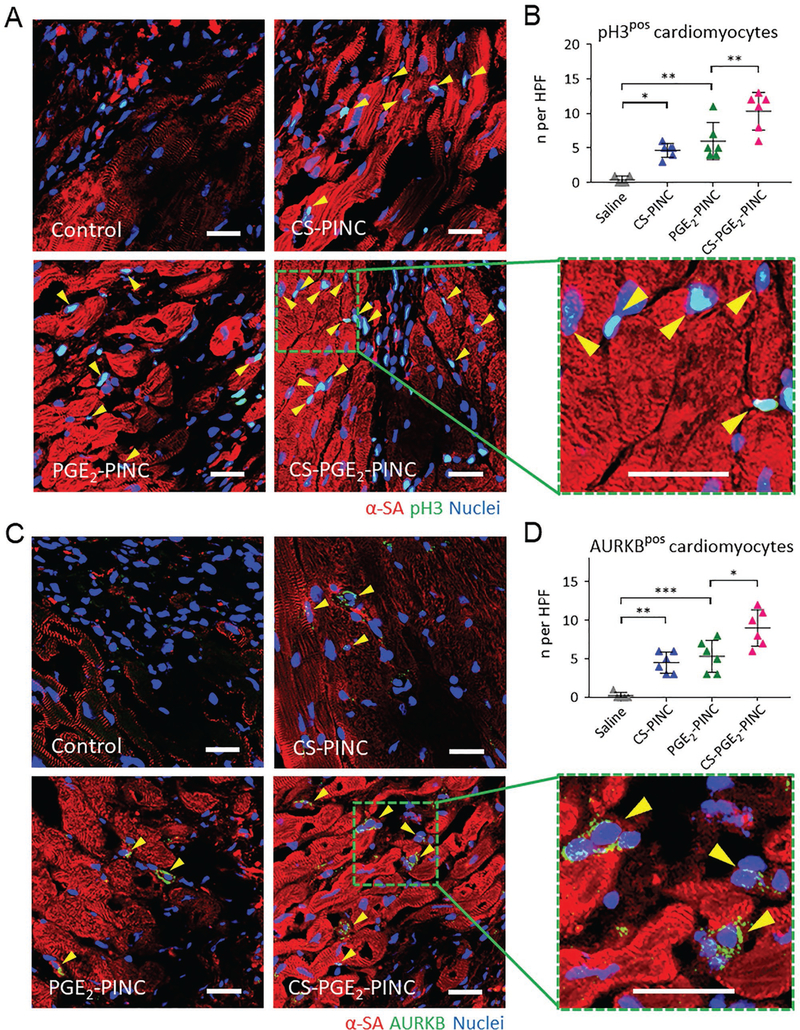
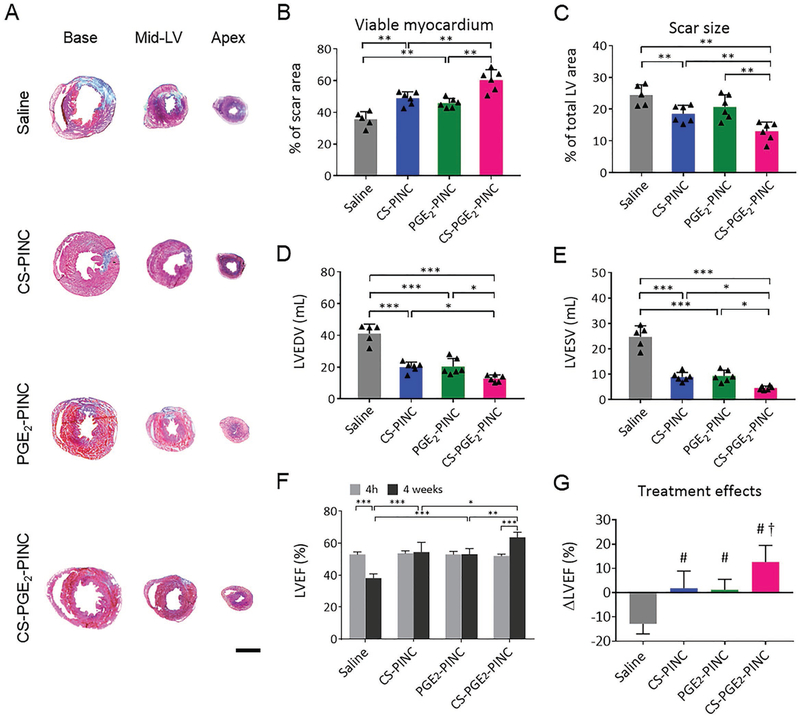
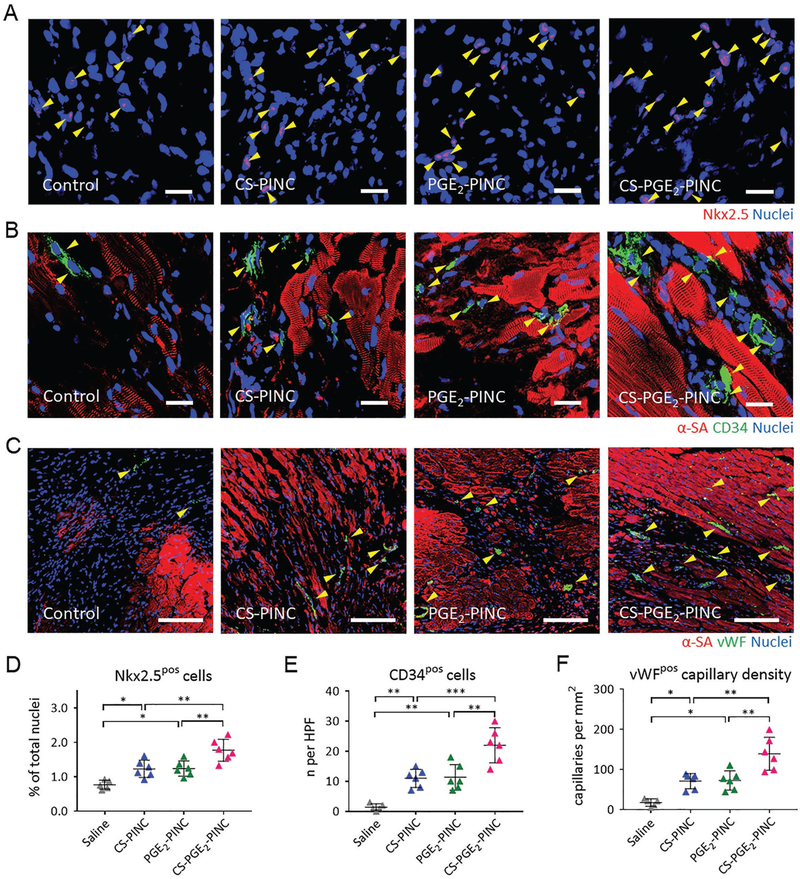
Cardiovascular disease is the leading cause of mortality worldwide. While reperfusion therapy is vital for patient survival post-heart attack, it also causes further tissue injury, known as myocardial ischemia/reperfusion (I/R) injury in clinical practice. Exploring ways to attenuate I/R injury is of clinical interest for improving post-ischemic recovery. A platelet-inspired nanocell (PINC) that incorporates both prostaglandin E2 (PGE2)-modified platelet membrane and cardiac stromal cell-secreted factors to target the heart after I/R injury is introduced. By taking advantage of the natural infarct-homing ability of platelet membrane and the overexpression of PGE2 receptors (EPs) in the pathological cardiac microenvironment after I/R injury, the PINCs can achieve targeted delivery of therapeutic payload to the injured heart. Furthermore, a synergistic treatment efficacy can be achieved by PINC, which combines the paracrine mechanism of cell therapy with the PGE2/EP receptor signaling that is involved in the repair and regeneration of multiple tissues. In a mouse model of myocardial I/R injury, intravenous injection of PINCs results in augmented cardiac function and mitigated heart remodeling, which is accompanied by the increase in cycling cardiomyocytes, activation of endogenous stem/progenitor cells, and promotion of angiogenesis. This approach represents a promising therapeutic delivery platform for treating I/R injury.
Keywords: biomimetics; drug delivery; ischemic injury; platelets; stromal cell secretome.
Conflict of interest statement
Conflict of Interest The authors declare no conflict of interest.
Figures
References
-
- Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M, Eur. Heart J 2016, 37, 3232. - PubMed
-
- Chouchani ET, Pell VR, Gaude E, Aksentijevic D, Sundier SY, Robb EL, Logan A, Nadtochiy SM, Ord ENJ, Smith AC, Eyassu F, Shirley R, Hu C-H, Dare AJ, James AM, Rogatti S, Hartley RC, Eaton S, Costa ASH, Brookes PS, Davidson SM, Duchen MR, Saeb-Parsy K, Shattock MJ, Robinson AJ, Work LM, Frezza C, Krieg T, Murphy MP, Nature 2014, 515, 431. - PMC - PubMed
-
- Bolli R, Ghafghazi S, Nat. Rev. Cardiol 2017, 14, 257. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources