

Function and Psychotherapy of Chronic Suicidality in Borderline Personality Disorder: Using the Reinforcement Model of Suicidality
- PMID: 32256412
- PMCID: PMC7093558
- DOI: 10.3389/fpsyt.2020.00199
Function and Psychotherapy of Chronic Suicidality in Borderline Personality Disorder: Using the Reinforcement Model of Suicidality
Abstract
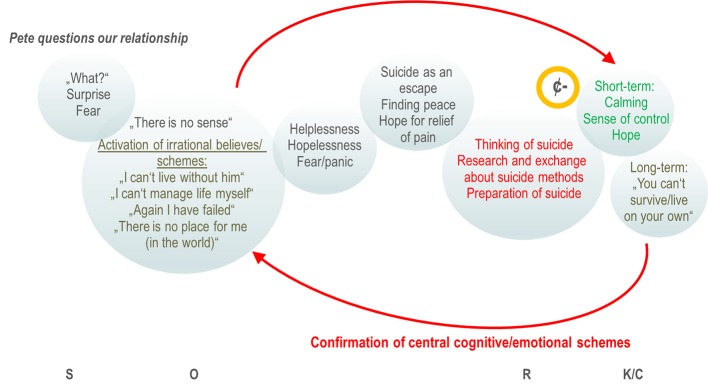
Although great advancements in evidence-based therapies, chronic suicidal patients with borderline personality disorder (BPD) still challenge our mental health system. While BPD patients continue suffering from distress and aversive emotions, therapists and relatives feel often stunned and helpless when confronted with suicidality resulting in interruption of therapies, repeated presentations to emergency rooms and referrals to hospitals. Reviewing the current knowledge of the functions and background of non-suicidal self-injury, we learned that reinforcement mechanisms play an important role to understand why individuals act in deliberate self-mutilation. While individual motives for non-suicidal self-injury and suicidal behavior including suicidal ideations can differ, the principle mechanisms appear to be transferrable. Elucidating the individual motives and function of suicidal behavior is an important therapeutic step, giving us access to very central maladaptive schemes and false believes that we need to address in order to reduce chronic suicidality in BPD patients. This Perspective article aims to give a better idea of what is behind and what are the differences between non-suicidal self-injury, suicidal ideations and suicide attempts. It further integrates recent developments of behavioral science in a reinforcement model of suicidality that can provide therapists a practical armamentarium in their work with chronic suicidal clients.
Keywords: DBT; behavioral analysis; borderline personality disorder; non-suicidal self-injury; psychotherapy; reinforcement; suicidality; suicide attempt.
Copyright © 2020 Hennings.
Figures
Similar articles
-
[Borderline personality disorder, self-mutilation and suicide: literature review].Encephale. 2008 Oct;34(5):452-8. doi: 10.1016/j.encep.2007.10.007. Epub 2008 Feb 20. Encephale. 2008. PMID: 19068333 Review. French.
-
Sub-clinical borderline personality disorder symptoms as predictor of suicidality and non-suicidal self-injury in young Pakistani females.J Pak Med Assoc. 2021 Feb;71(2(B)):740-743. doi: 10.47391/JPMA.1088. J Pak Med Assoc. 2021. PMID: 33941971
-
Therapists' emotional state after sessions in which suicidality is addressed: need for improved management of suicidal tendencies in patients with borderline personality pathology.BMC Psychiatry. 2021 Nov 23;21(1):590. doi: 10.1186/s12888-021-03549-9. BMC Psychiatry. 2021. PMID: 34814860 Free PMC article.
-
Frequent follow-up of suicidal youth assessed in the emergency room: Long-term trajectory and predictors of suicidality.Prev Med. 2021 Nov;152(Pt 1):106737. doi: 10.1016/j.ypmed.2021.106737. Epub 2021 Sep 16. Prev Med. 2021. PMID: 34538378
-
Nightmares in borderline personality disorder - narrative review.Neuro Endocrinol Lett. 2023 Jun 14;44(3):164-174. Neuro Endocrinol Lett. 2023. PMID: 37392443 Review.
Cited by
-
Suicidality, resilience and burnout in a population of oncology nurses.Sci Rep. 2025 Jan 25;15(1):3251. doi: 10.1038/s41598-025-87677-2. Sci Rep. 2025. PMID: 39863765 Free PMC article.
-
Chronic suicidal ideations: a risk or a protection.Res Psychother. 2024 Jun 19;27(3):764. doi: 10.4081/ripppo.2024.764. Res Psychother. 2024. PMID: 38904642 Free PMC article.
-
Recurrent suicide attempts affect normalization of HPA axis dysregulation after recovery from major depression.Front Psychiatry. 2022 Aug 12;13:937582. doi: 10.3389/fpsyt.2022.937582. eCollection 2022. Front Psychiatry. 2022. PMID: 36032226 Free PMC article.
References
-
- Miller AB, Eisenlohr-Moul T, Giletta M, Hastings PD, Rudolph KD, Nock MK. Prinstein MJ. A within-person approach to risk for suicidal ideation and suicidal behavior: Examining the roles of depression, stress, and abuse exposure. J Consult Clin Psychol (2017) 85:712–22. 10.1037/ccp0000210 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources