

Size and Shape of Associations of OGTT as Well as Mediating Effects on Adverse Pregnancy Outcomes Among Women With Gestational Diabetes Mellitus: Population-Based Study From Southern Han Chinese
- PMID: 32256449
- PMCID: PMC7092640
- DOI: 10.3389/fendo.2020.00135
Size and Shape of Associations of OGTT as Well as Mediating Effects on Adverse Pregnancy Outcomes Among Women With Gestational Diabetes Mellitus: Population-Based Study From Southern Han Chinese
Abstract
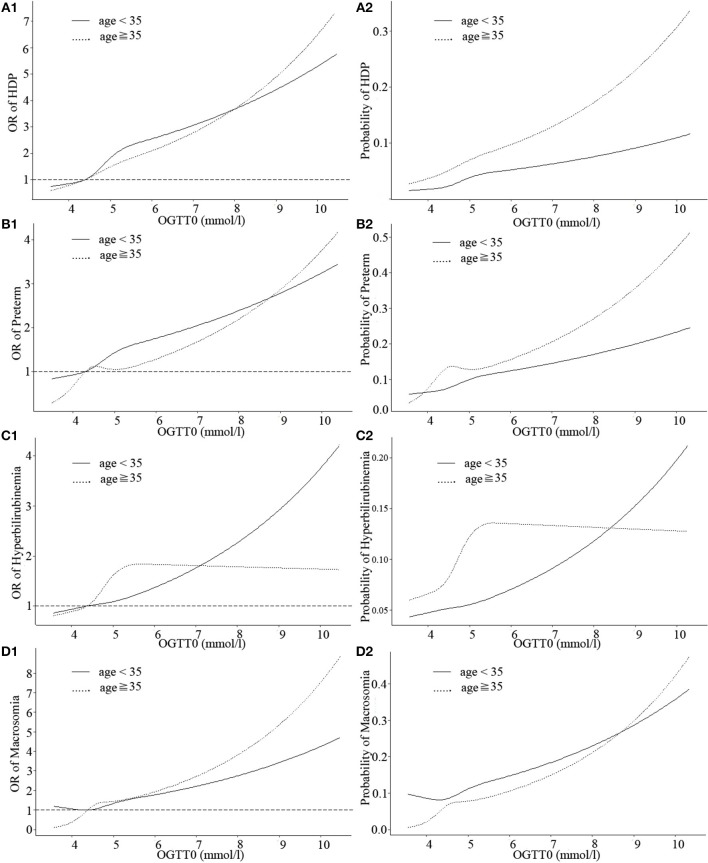
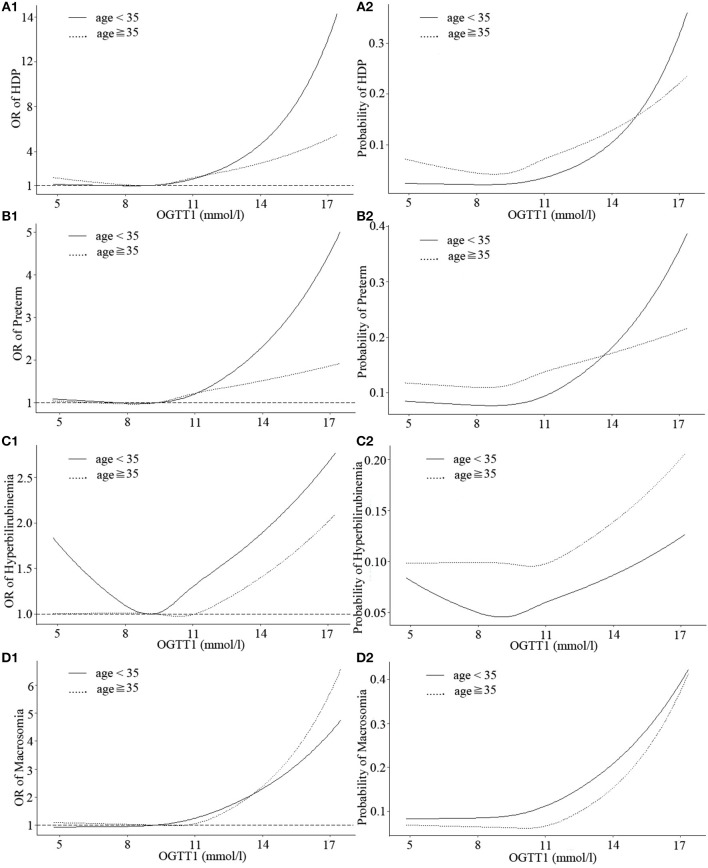
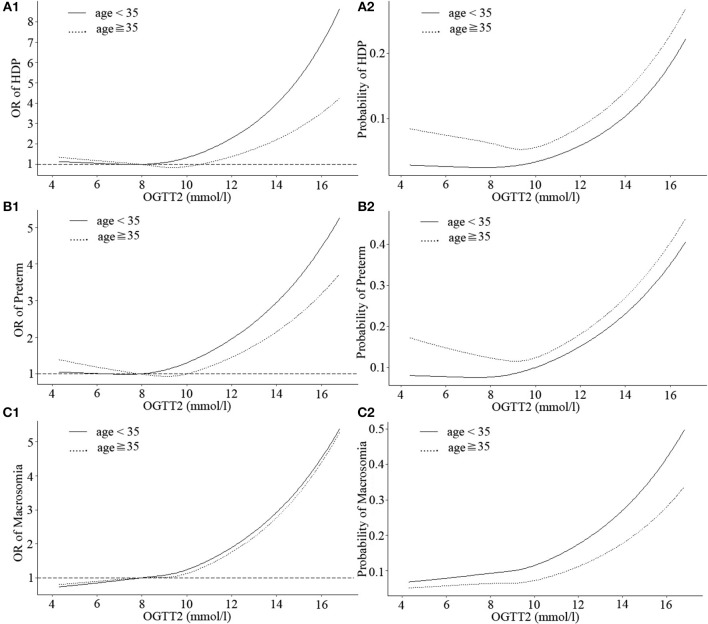
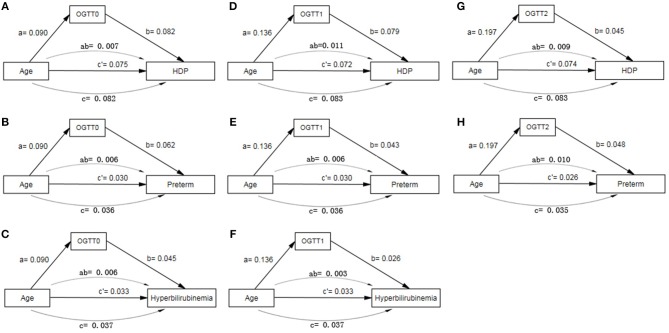
Objective: To explore the size and shape association of OGTT values with adverse pregnancy complications among women with gestational diabetes mellitus (GDM) in Southern Han Chinese population and further analyze their mediating effects with maternal age in outcomes. Methods: 6,861 women with GDM were included in the study. Logistic regression was used to identify the correlations between OGTT values and adverse pregnancy outcomes of GDM. Restricted cubic spline nested logistic regression was conducted to investigate potential non-linear and linear associations. Mediating effect among maternal age, OGTT and adverse outcomes were explored. Results: Women with GDM had a mean age of 31.83, and 24.49% had advanced maternal age (≥35 years). In logistic regression with adjustment, compared with lower OGTT0 (<5.1 mmol/L), GDM patients with higher OGTT0 (≥5.1 mmol/L) exhibited 1.891 (95% CI: 1.441-2.298, P < 0.001), 1.284 (1.078-1.529, P = 0.005), 1.285 (1.065-1.550, P = 0.009), and 1.302 (1.067-1.590, P = 0.010) times increased risk of hypertensive disorders of pregnancy (HDP), preterm, neonatal hyperbilirubinemia, and macrosomia, respectively. GDM patients with higher OGTT1 (≥10 mmol/L) had only found to exhibited 1.473-fold (1.162-1.867, P = 0.001) increasing risk of HDP than those with lower OGTT1 (<10 mmol/L). No adverse outcome was identified to associate with higher OGTT2 (≥8.5 mmol/L). Linear relationships (non-linear P > 0.05) were observed between OGTT0 and HDP, preterm, neonatal hyperbilirubinemia, and macrosomia in both maternal age groups (<35 and ≥35 years). Non-linear associations of OGTT1 with incidence of HDP, preterm, and neonatal hyperbilirubinemia were detected in GDM patients younger than 35 years (non-linear P = 0.037, P = 0.049, P = 0.039, respectively), rising more steeply at higher values. Similar non-linearity was noted for OGTT2 with HDP in older patients. All OGTT values had significant mediating effects on some special complications caused by higher age. Conclusion: Higher fasting plasma glucose was more strongly linked to adverse pregnancy outcomes among GDM patients. Both linearity and Non-linearity of associations between glucose and complications should be taken into account. A careful reconsideration of GDM with hierarchical and individualized management according to OGTT is needed.
Keywords: OGTT; adverse pregnancy outcomes; gestational diabetes mellitus; mediating effect; restricted cubic spline.
Copyright © 2020 Zhou, Chen, Fan, Rao, Li, Wu, Lin, Ma, Ye, Zhang, Shen, Wan, Luo, Suo, Guo and Liu.
Figures
References
-
- International Diabetes Federation IDF Diabetes Atlas. 8th ed Brussels: International Diabetes Federation: (2017).
-
- Lappin TR J. Hyperglycemia and adverse pregnancy outcomes the HAPO study cooperative research group*. Obstetr Gynecol Survey. (2008) 63:1991 10.1097/OGX.0b013e318187b7a2 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical