

Fast-track extubation in patients after intracranial hematoma surgery
- PMID: 32256735
- PMCID: PMC7098210
- DOI: 10.3892/etm.2020.8507
Fast-track extubation in patients after intracranial hematoma surgery
Abstract
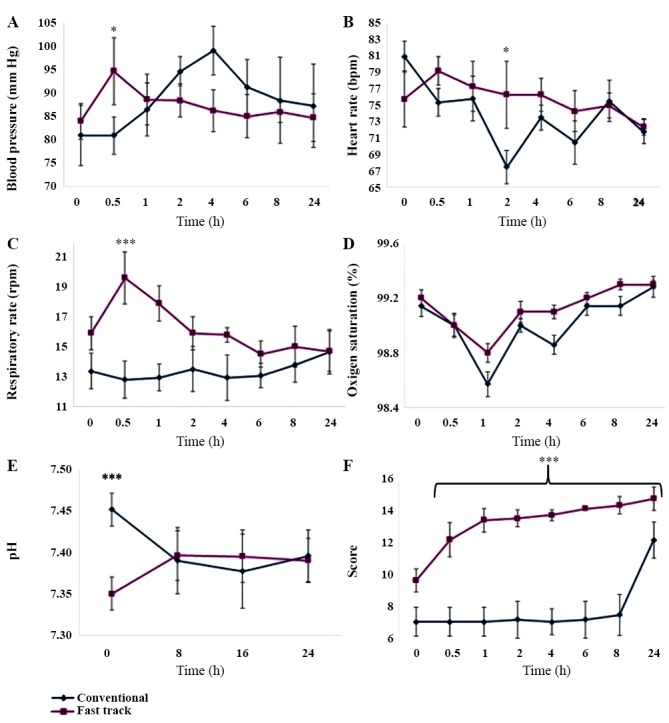
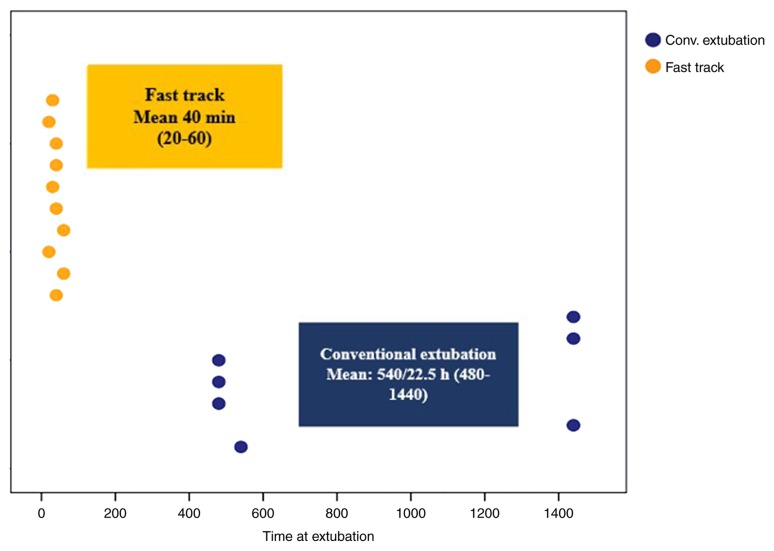
Early extubation, also known as fast track, is desirable after intracranial hematoma surgery to avoid ventilator-associated complications associated with admission to an intensive care unit (ICU). The objective of the present study was to determine whether ICU stay and ventilator-associated complications are reduced in patients who received surgery for intracranial hematoma if they are extubated early. A total of 17 patients were randomly assigned to two groups: In Group 1, patients were extubated early or using the fast track method, while those in Group 2 were conventionally extubated at a later stage and were managed at the ICU. Patients from both groups were assessed on admission to the operating room per the established standards and after the selection criteria had been confirmed, general anesthesia was applied. Extubation time and hemodynamic stability (number of anesthetic adjustments required to maintain hemodynamic parameters within 20% of the predicted values) were assessed post-operatively. Patients in the conventional group (n=10) were transferred to the ICU and extubated at 8 h post-operatively; hemodynamic stability and the presence of complications were evaluated. The fast track group had no complications associated with ventilation or any other parameter. All patients extubated in a conventional manner and who were transferred to the ICU presented with complications, including seizures, aspiration, atelectasis or failed extubation. In the future, fast track should be regarded as a routine technique in patients who meet the required criteria, so that they may be discharged quickly and with fewer complications. The present study was authorized by the ethics committee of the hospital and the research sub-directorate with the number AN14-003; it was submitted to and approved by the ISRCTN registry for clinical trials (ID, ISRCTN16924441).
Keywords: avoidance of complications; fast track; intensive care unit; intracranial hematoma; post-surgery patients.
Copyright: © González-Cordero et al.
Figures
References
-
- Henao FA, Restrepo CE, Botero LF, Arango MF, Jaramillo AF. Extubación temprana (fast-track) en neuroanestesia: Una alternativa segura? Rev Col Anest. 2004;32:179–184.
-
- González-Villavelázquez ML, Castelazo-Arredondo JA, Osorio-Santiago MA. Extubación temprana en neurocirugía. Revista Mexicana de Anestesiología. Neuroanestesiología. 2005;28 (Suppl 1):S120–S112.
LinkOut - more resources
Full Text Sources