

The efficacy and adverse effects of the Uniblocker and left-side double-lumen tube for one-lung ventilation under the guidance of chest CT
- PMID: 32256757
- PMCID: PMC7086194
- DOI: 10.3892/etm.2020.8492
The efficacy and adverse effects of the Uniblocker and left-side double-lumen tube for one-lung ventilation under the guidance of chest CT
Abstract
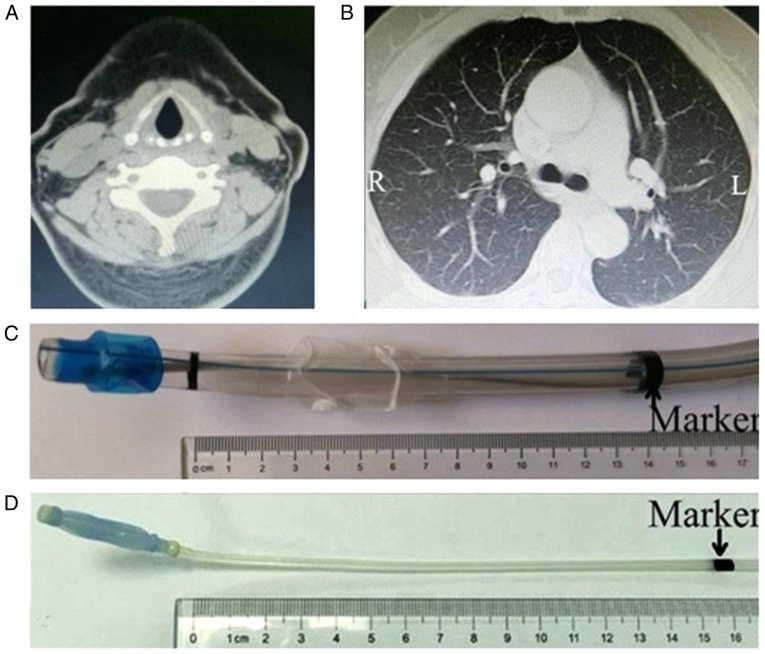
One-lung ventilation (OLV) is essential in numerous clinical procedures, in which the left-sided double-lumen tube (LDLT) is the most commonly used device. The application of bronchial blockers, including the Uniblocker or Arndt blocker, has increased in OLV. The present study aimed to compare the efficacy and adverse effects of the Uniblocker and LDLT for OLV under the guidance of chest CT. A total of 60 adult patients undergoing elective left-side thoracic surgery requiring OLV were included in the study. The patients were randomly assigned to the Uniblocker group (U group, n=30) or the LDLT group (D group, n=30). The time for initial tube placement, the number of optimal positions of the tube upon blind insertion, the number of attempts to adjust the tube to the optimal position, incidence of airway device displacement, injury to the bronchi and carina, the duration until lung collapse and the occurrence of sore throat and hoarseness over 24 h following surgery were recorded. The time for successful placement of the LDLT was 83.9±19.4 sec and that for the Uniblocker was 84.3±17.1 sec (P>0.05). The degree of lung collapse 1 min following opening of the pleura was greater in the D group than that in the U group (P<0.01) and the time required for the lung to completely collapse was shorter in the D group (3.3±0.5 min) than that in the U group (8.4±1.2 min; P<0.01). On the contrary, the incidence of injury to the bronchi and carina was lower in the U group (2/30 cases) than in the D group (10/30 cases; P=0.02); the incidence of sore throat was also lower in the U group (2/30 cases) compared with that in the D group (9/30 cases). The mean arterial pressure of patients immediately following intubation was lower in the U group (122.0±13.4 mmHg) than that in the D group (129.2±12.1 mmHg; P<0.05). The results of the present study indicated that the extraluminal use of the Uniblocker under guidance of chest CT is an efficient method with few adverse effects in left-side thoracic surgery. The study was registered at ClinicalTrials.gov on 16th December 2017 (no. NCT03392922).
Keywords: Uniblocker; double-lumen tube; intubation; thoracic surgery.
Copyright © 2020, Spandidos Publications.
Figures

References
Associated data
LinkOut - more resources
Full Text Sources
Medical