

Surgery for the Pronated Forearm and Flexed Wrist in Children with Cerebral Palsy
- PMID: 32257022
- PMCID: PMC7093635
- DOI: 10.1007/s43465-019-00021-5
Surgery for the Pronated Forearm and Flexed Wrist in Children with Cerebral Palsy
Abstract
Aim: There is no consensus in the literature on how best to manage wrist flexion and forearm pronation deformities in children with cerebral palsy (CP). The aim of this research was to come up with a treatment algorithm for the surgical management of such cases.
Methods: Children with CP who underwent upper limb surgery between 2009 and 2016 at a single centre and by a single lead surgeon were reviewed retrospectively. Movement analysis and Shriners Hospital Upper Extremity Evaluation (SHUEE) data collected pre- and post-operatively.
Results: Thirteen patients were recruited. Most patients underwent a flexor carpi ulnaris (FCU) to extensor carpi radialis brevis (ECRB) transfer, with or without pronator teres (PT) re-routing, and finger flexor or elbow flexor releases. Mean increase in active range of supination was 40.8° (p = 0.002) and wrist extension 28.9° (p = 0.004). The mean increase in dynamic positional analysis (part of the SHUEE) was 25.4% (of which 40.3% was due the increases in wrist function and 16.8% due to forearm function). The loss of wrist flexion was not significant (p = 0.125). The mean follow-up was 14 months (range 9-21).
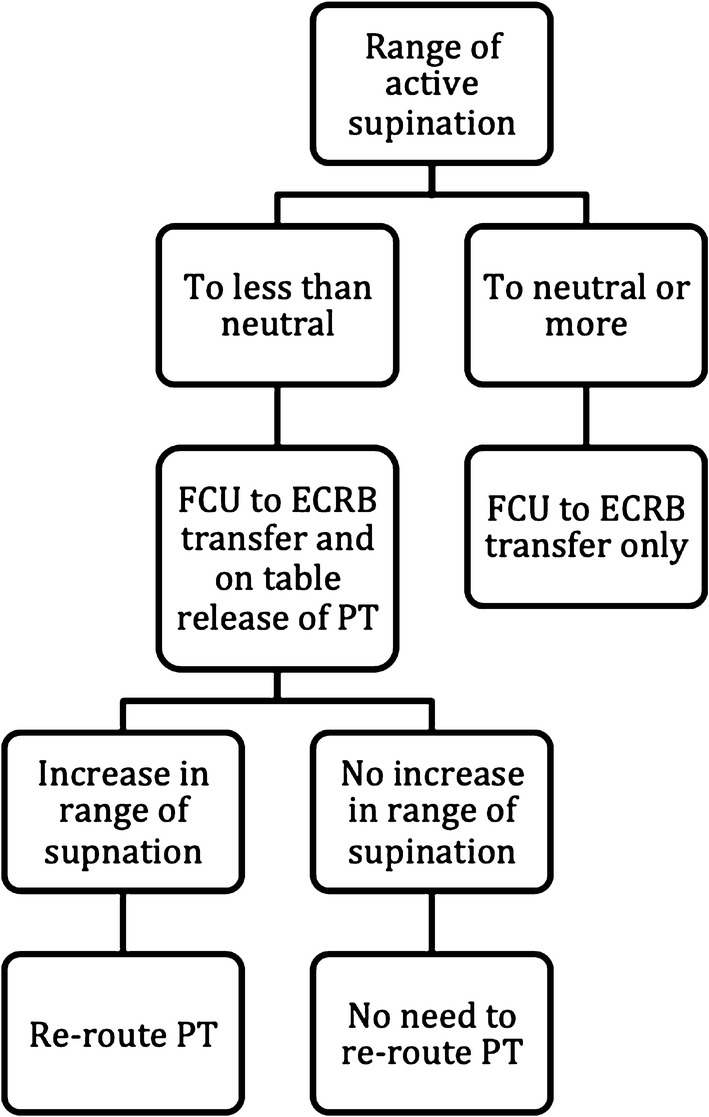
Conclusions: To tackle both a pronation and flexion deformity, the authors favour performing a FCU to ECRB transfer in isolation if there is active supination to neutral; if active supination is short of neutral, then a FCU to ECRB with a PT release and possible re-routing performed. A treatment algorithm is proposed.
Level of evidence: IV.
Keywords: Cerebral palsy; ECRB; FCU; Flexion; Movement analysis; Paediatrics; Pronation; Surgery.
© Indian Orthopaedics Association 2020.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures
References
-
- Kreulen M, Smeulders M, Veeger H, Hage J. Movement patterns of the upper extremity and trunk before and after corrective surgery of impaired forearm rotation in patients with cerebral palsy. Developmental Medicine and Child Neurology. 2006;48(6):436–441. doi: 10.1017/S0012162206000958. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous