

Colorectal cancer screening: Assessment of CEACAM6, LGALS4, TSPAN8 and COL1A2 as blood markers in faecal immunochemical test negative subjects
- PMID: 32257432
- PMCID: PMC7113625
- DOI: 10.1016/j.jare.2020.03.001
Colorectal cancer screening: Assessment of CEACAM6, LGALS4, TSPAN8 and COL1A2 as blood markers in faecal immunochemical test negative subjects
Abstract
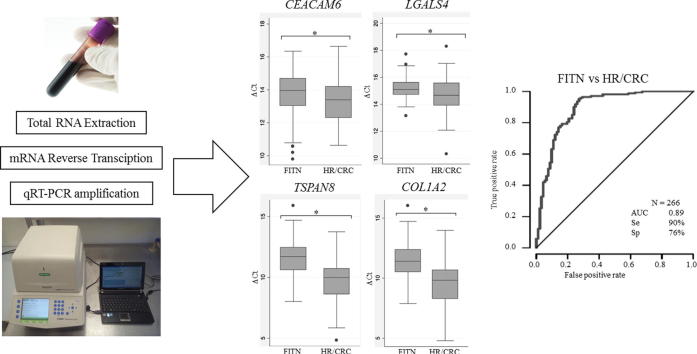
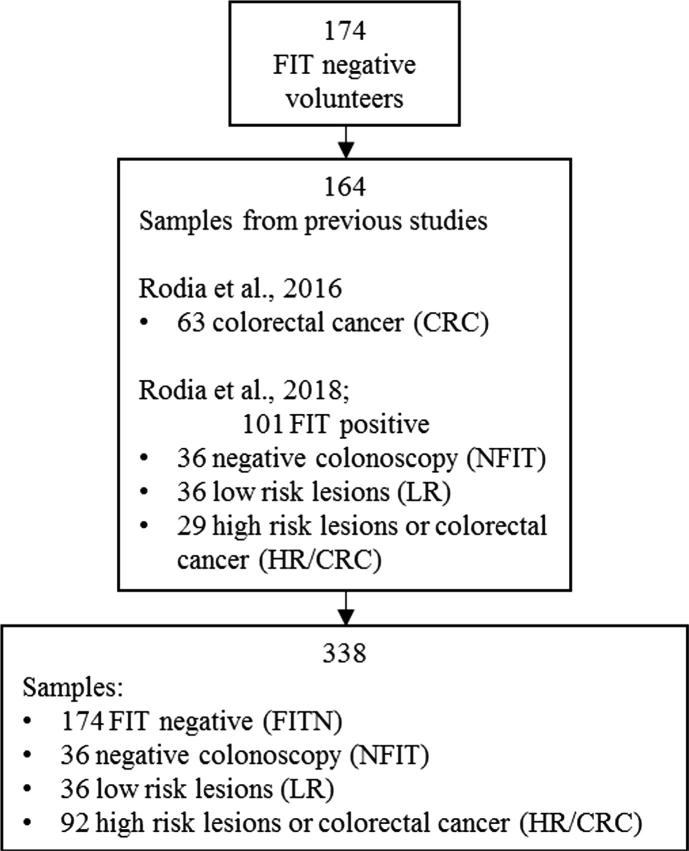
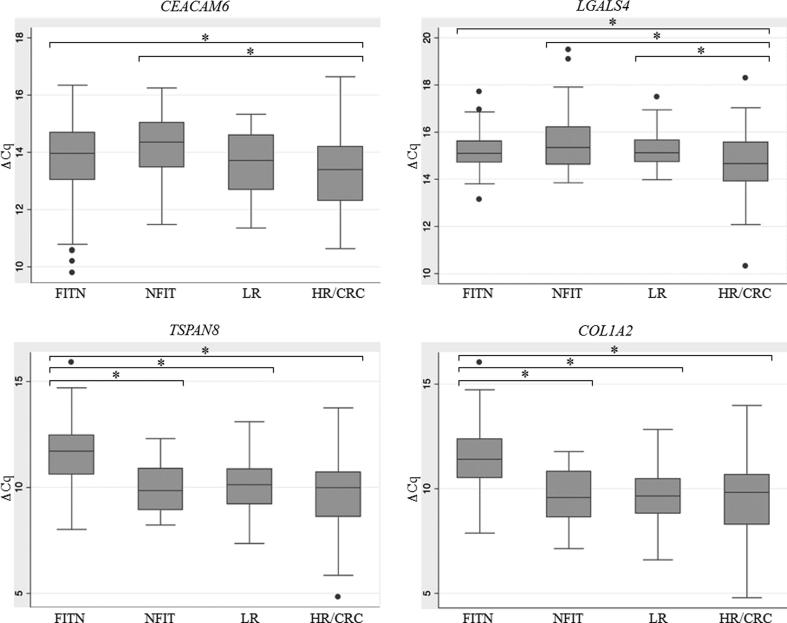
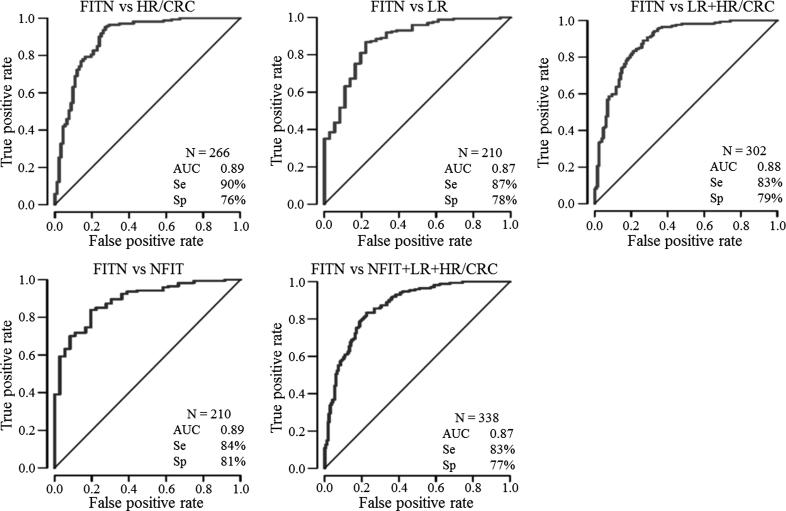
Prevention is essential to reduce Colorectal Cancer (CRC) mortality. We previously reported a panel of four genes: CEACAM6, LGALS4, TSPAN8, COL1A2 (CELTiC) able to discriminate patients with CRC. Here, we assessed the CELTiC panel by quantitative polymerase chain reaction, in the blood of 174 healthy subjects, who resulted negative to the faecal immunochemical test (FITN). Using non-parametric statistic and multinomial logistic models, the FITN were compared to previously analysed subjects: 36 false positive FIT (NFIT), who were negative at colonoscopy, 36 patients with low risk lesions (LR) and 92 patients with high risk lesions or CRC (HR/CRC). FITN showed a significantly lower expression of the four genes when compared to HR/CRC. Moreover, FITN showed a significantly lower expression of TSPAN8 and COL1A2 compared to NFIT and LR patients. The multinomial logistic model confirmed that TSPAN8 alone specifically discriminated FITN from NFIT, LR and HR/CRC, while LGALS4 was able to differentiate FITN from false positive FIT. Finally, ROC curves analysis of the comparisons between FITN and HR/CRC, LR or NFIT reported AUC greater than 0.87, with a sensitivity and specificity of 83% and 76%, respectively. The CELTiC panel was confirmed a useful tool to identify CRC patients and to discriminate false FIT positive subjects.
Keywords: Blood mRNA; CEACAM6; COL1A2; Faecal immunochemical test; LGALS4; TSPAN8.
© 2020 THE AUTHORS. Published by Elsevier BV on behalf of Cairo University.
Figures
References
-
- Ferlay J., Colombet M., Soerjomataram I., Mathers C., Parkin D.M., Piñeros M. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. - PubMed
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Senore C., Basu P., Anttila A., Ponti A., Tomatis M., Vale D.B. Status of implementation and organization of cancer screening in The European Union Member States—Summary results from the second European screening report. Int J Cancer. 2018;142:44–56. - PubMed
-
- Benson V.S., Atkin W.S., Green J., Nadel M.R., Patnick J., Smith R.A. Toward standardizing and reporting colorectal cancer screening indicators on an international level: the international colorectal cancer screening network. Int J Cancer. 2012;130:2961–2973. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
