

Orbital myxoma: A case report
- PMID: 32257569
- PMCID: PMC7110406
- DOI: 10.25259/SNI_323_2019
Orbital myxoma: A case report
Abstract
Background: Myxomas are rare, locally infiltrative, benign neoplasms of mesenchymal origin. Although benign, these tumors are locally aggressive with a high rate of recurrence following conservative resection. Their relative infrequency, variable location, and insidious growth present a diagnostic challenge to clinicians. Cases of myxomas have been described throughout the body, but intraosseous myxomas of the orbit are exceedingly rare.
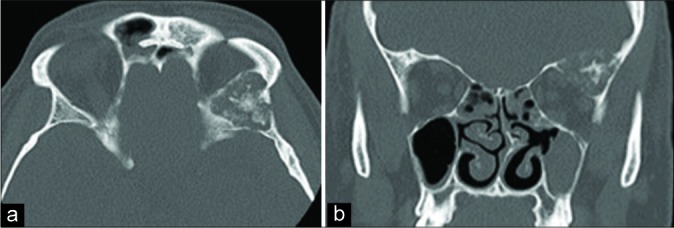
Case description: We report a case of a 53-year-old male with a history of chronic sinusitis and symptoms of hyposmia and bifrontal headaches refractory medical management who presented for neurosurgical evaluation after radiographic findings of an orbital lesion. Physical examination was unremarkable with intact extraocular movements. Prior radiographic workup demonstrated a 2.4 × 2.7 × 2.2 cm expansile lesion involving the bony left superior and lateral orbit. A prior open biopsy was performed which demonstrated a low-grade spindle cell neoplasm consistent with intraosseous myxoma. Definitive resection was recommended through the left orbitozygomatic craniotomy. The patient tolerated the procedure well without complications. Gross total resection was achieved. Reconstruction of the orbital roof and lateral orbital wall was performed with a frontal bone autograft and titanium plating. Postoperative course was uneventful, and the patient was discharged home postoperative day 2. At 1-month follow-up visit, the patient remained neurologically intact. Surveillance imaging at 6 months and 1 year remained stable without signs of recurrence.
Conclusion: Intraosseous orbital myxomas are exceedingly rare entities. Although they are considered benign neoplasms, myxomas demonstrate high recurrence rates. The authors report a unique case of an orbital myxoma that was successfully treated through an orbitozygomatic approach achieving gross total resection.
Keywords: Intraosseous; Myxoma; Orbit.
Copyright: © 2020 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Andrews T, Kountakis SE, Maillard AA. Myxomas of the head and neck. Am J Otolaryngol. 2000;21:184–9. - PubMed
-
- Bajaj MS, Mehta M, Kashyap S, Pushker N, Lohia P, Chawla B, et al. Clinical and pathologic profile of angiomyxomas of the orbit. Ophthalmic Plast Reconstr Surg. 2011;27:76–80. - PubMed
-
- Batsakis JG. Myxomas of soft tissues and the facial skeleton. Ann Otol Rhinol Laryngol. 1987;96:618–9. - PubMed
-
- Candy EJ, Miller NR, Carson BS. Myxoma of bone involving the orbit. Arch Ophthalmol. 1991;109:919–20. - PubMed
-
- Court-Payen M, Ingemann Jensen L, Bjerregaard B, Schwarz Lausten G, Skjoldbye B. Intramuscular myxoma and fibrous dysplasia of bone--mazabraud’s syndrome. A case report. Acta Radiol. 1997;38:368–71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources