

Computed Tomography-based Diagnosis of Post-laparoscopic Sleeve Gastrectomy Gastric Leak
- PMID: 32257584
- PMCID: PMC7109466
- DOI: 10.25259/JCIS_5_2020
Computed Tomography-based Diagnosis of Post-laparoscopic Sleeve Gastrectomy Gastric Leak
Abstract
Objective: Gastric leak post-laparoscopic sleeve gastrectomy may appear as a variety of computed tomography (CT) findings. We aimed to review the various CT findings sensitivity and specificity in confirmed cases of gastric leak.
Materials and methods: A retrospective review was performed for all patients who underwent sleeve gastrectomy, CT, and endoscopy for suspected leak between 2011 and 2018. All patients with positive CT findings for gastric leak were included in the study.
Results: A total of 152 consecutive patients underwent CT for suspected post-sleeve gastrectomy gastric leak. Out of 152 patients, 88 had positive CT findings for gastric leak and underwent endoscopy. The CT findings sensitivity and specificity of perigastric collection without oral contrast leak were 61% and 88.8%, oral contrast leak were 28% and 100%, and gas leak were 10% and 77.7%, respectively.
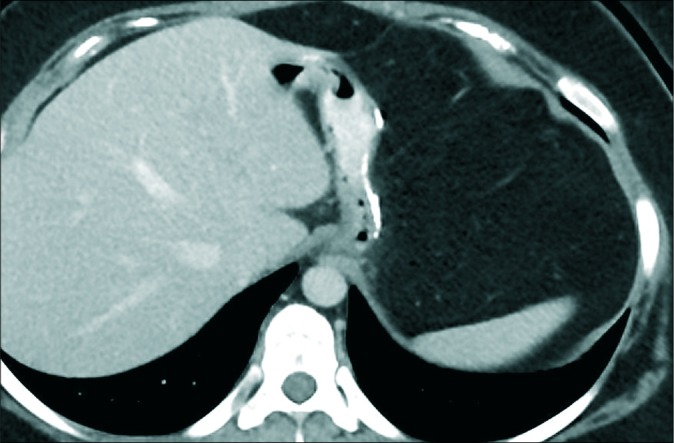
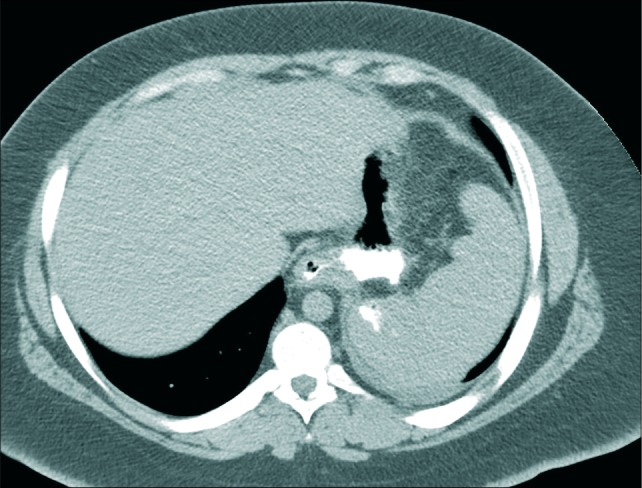
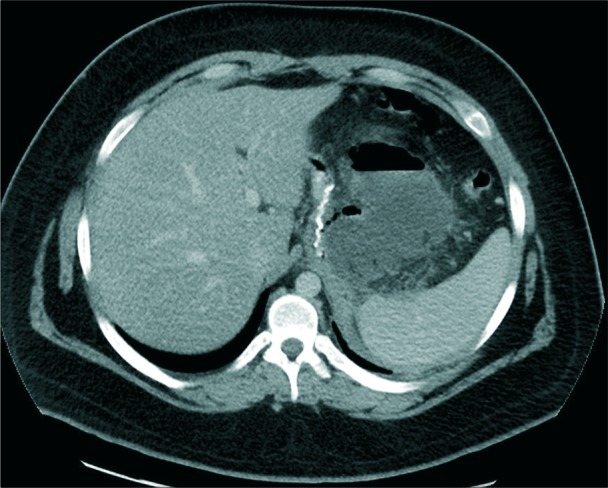
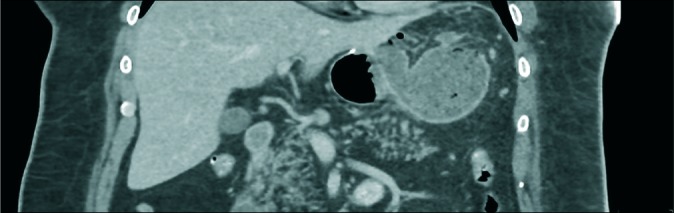
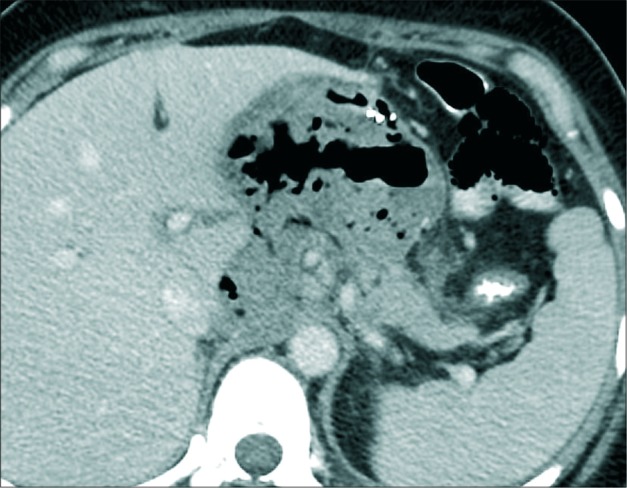
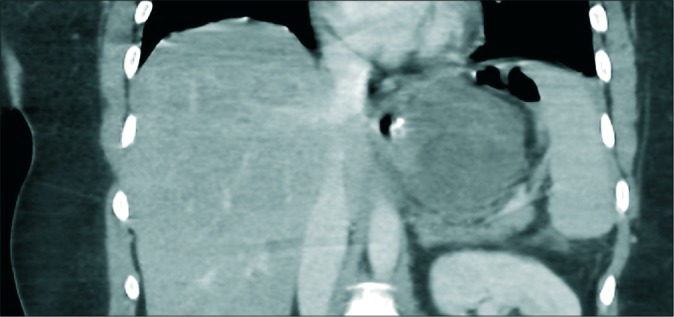
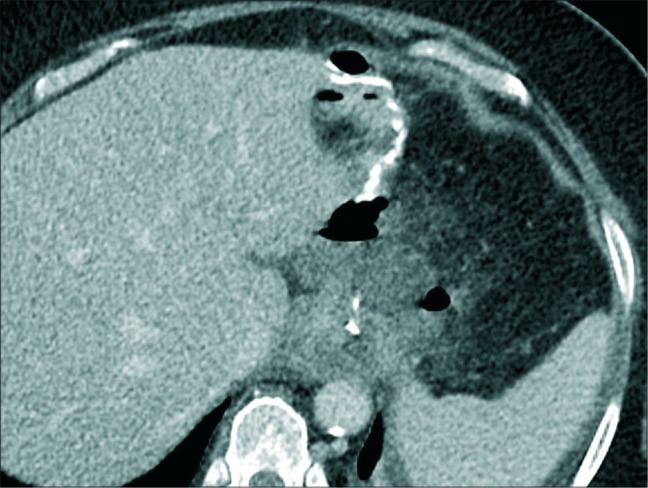
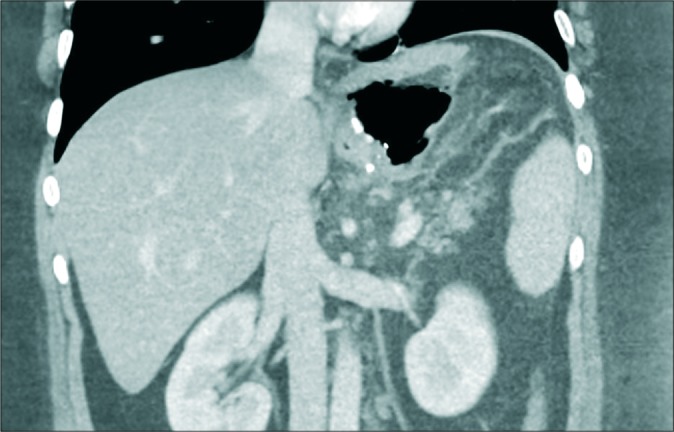
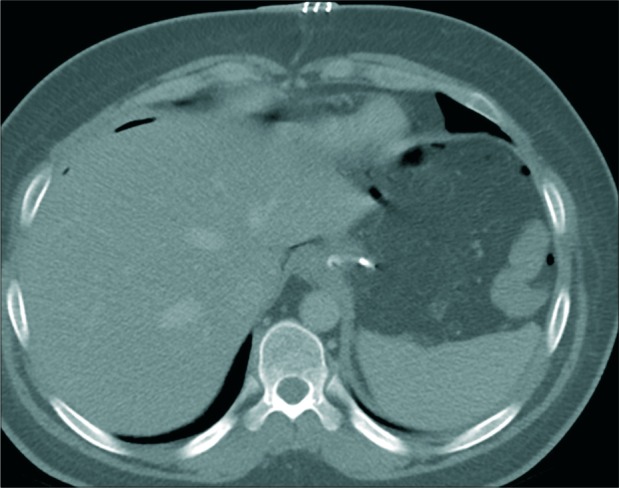
Conclusions: Perigastric fluid collection without contrast leak and with variable wall enhancement and gas content is the most common CT findings of post-sleeve gastrectomy gastric leak. Among various CT findings, it exhibits good diagnostic accuracy with 61% sensitivity and 88.8% specificity.
Keywords: Computed tomography; Gastric leak; Laparoscopic sleeve gastrectomy.
© 2020 Published by Scientific Scholar on behalf of Journal of Clinical Imaging Science.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
LinkOut - more resources
Full Text Sources