

Gross Total vs. Subtotal Resection on Survival Outcomes in Elderly Patients With High-Grade Glioma: A Systematic Review and Meta-Analysis
- PMID: 32257941
- PMCID: PMC7093492
- DOI: 10.3389/fonc.2020.00151
Gross Total vs. Subtotal Resection on Survival Outcomes in Elderly Patients With High-Grade Glioma: A Systematic Review and Meta-Analysis
Abstract
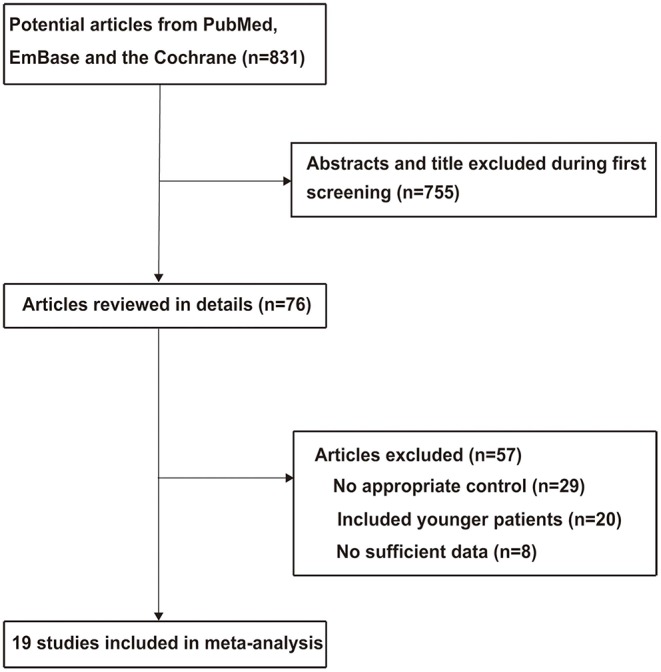
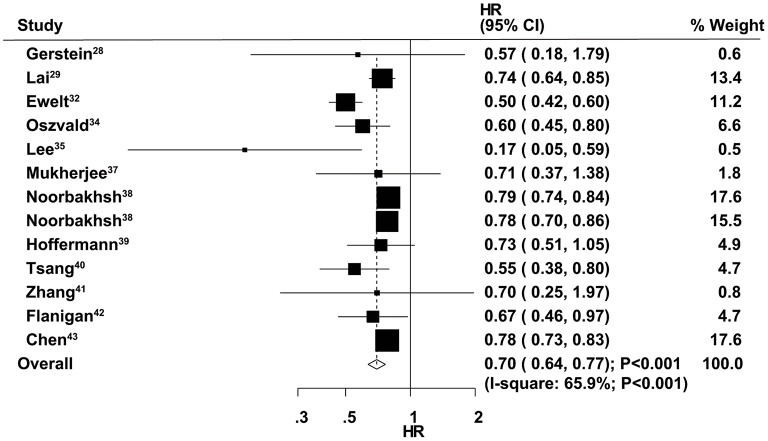
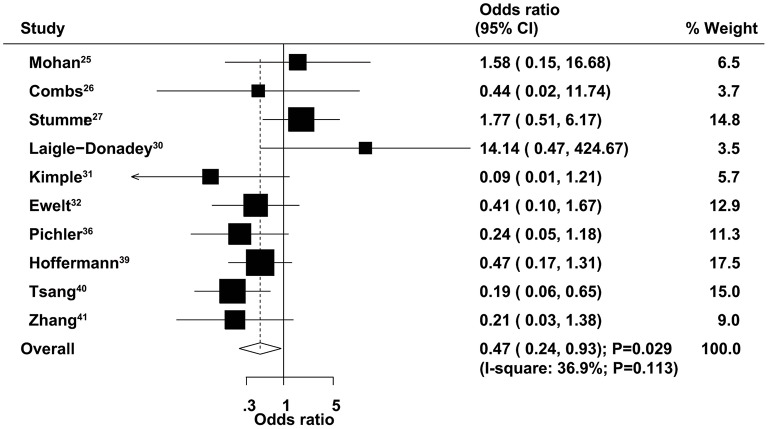
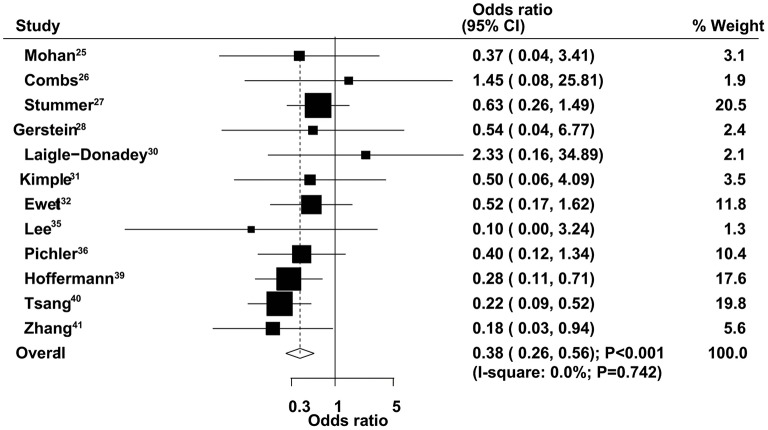
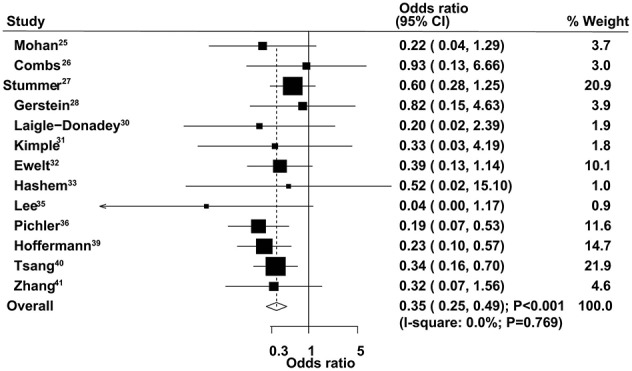
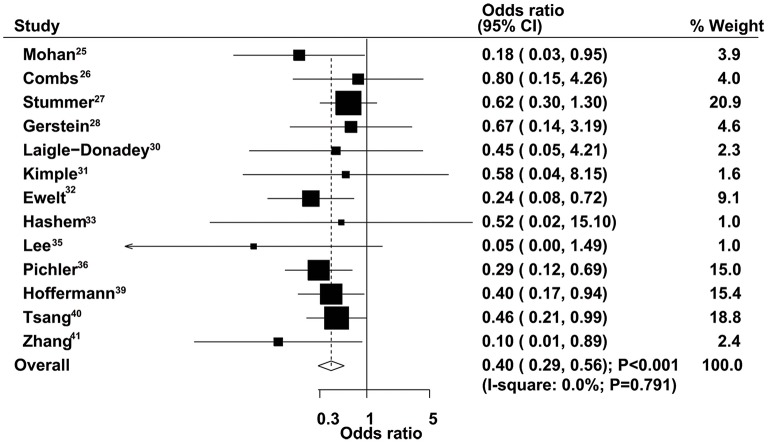
Background: The optimal strategy for the management of high-grade glioma in the elderly (≥60.0 years) remains controversial, especially regarding the effects of surgical extent on survival outcomes. The purpose of this study was to compare gross total resection (GTR) with subtotal resection (STR) for treatment effects in elderly patients with high-grade glioma. Methods: Three electronic databases were systematically searched, including PubMed, EmBase, and the Cochrane library, from inception to August 2018. Hazard ratios (HRs) or odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were used to express summary effect estimates using the random-effects model. Nineteen retrospective observational studies involving a total of 10,815 elderly patients with high-grade glioma were included in this meta-analysis. Results: The summary results indicated that GTR was associated with a significant improvement in overall survival (OS) compared with STR (HR = 0.70, 95% CI = 0.64-0.77). In addition, elderly patients administered GTR showed lower risk of 3-month mortality (OR = 0.47, 95% CI = 0.24-0.93), 6-month mortality (OR = 0.38, 95% CI = 0.26-0.56), 9-month mortality (OR = 0.35, 95% CI = 0.25-0.49), and 1-year mortality (OR = 0.40, 95% CI = 0.29-0.56). Pooled OS data differed when stratified by publication year, country, sample size, disease status, and study quality. Conclusion: GTR seems to be more effective than STR in achieving longer survival in elderly patients with high-grade glioma.
Keywords: elderly patients; gross total resection; high-grade glioma; meta-analysis; mortality; subtotal resection.
Copyright © 2020 Han, Liang, Cheng, Yang and Zhao.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, et al. . Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. (2009) 10459–66. 10.1016/S1470-2045(09)70025-7 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources