

Safety and efficacy of cabazitaxel in Japanese patients with castration-resistant prostate cancer
- PMID: 32257975
- PMCID: PMC7125373
- DOI: 10.1016/j.prnil.2019.10.005
Safety and efficacy of cabazitaxel in Japanese patients with castration-resistant prostate cancer
Abstract
Background: Several studies have reported the efficacy of cabazitaxel in cancer therapy; however, investigations of its safety are few. The aim of this study was to retrospectively analyze the efficacy and safety of cabazitaxel based on treatment outcome data.
Methods: A questionnaire form on the use of cabazitaxel was mailed to hospitals associated with the Shinshu University. Responses were received from 11 institutions regarding 55 cases.
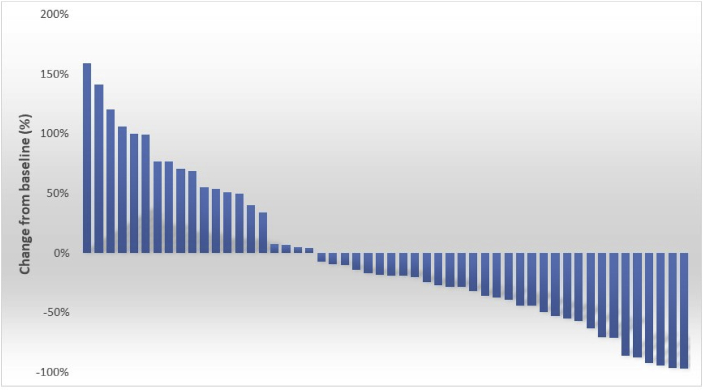
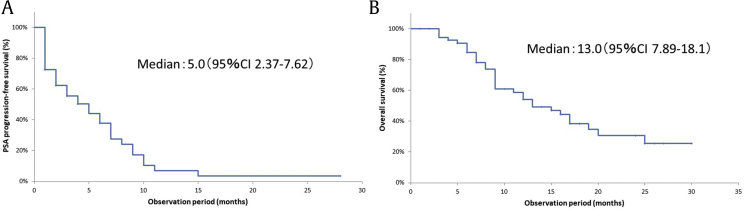
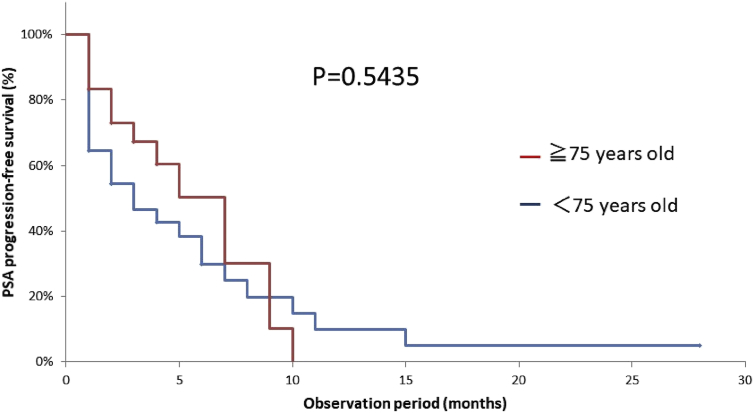
Results: Patients received a median of 4 courses of cabazitaxel treatment. Decreases in prostrate-specific antigen (PSA) were observed in 61.5% of cases with declines of 30%, 50%, and 90% in 36.5%, 23.0%, and 7.6% of cases, respectively. PSA progression-free survival was 5.0 months, and overall survival after the start of cabazitaxel was 13.0 months. Forty-five patients received postcabazitaxel treatment; 17 showed decreased PSA. Safety assessment indicated that white blood cell and neutrophil counts were significantly higher in the second than in the first course of treatment and Grade 3 to 4 leukopenia and neutropenia significantly decreased. Twenty-four subjects were aged ≥75 years; 79% of them had their doses reduced at the first administration. The mean dose was 20 mg/m2. However, there was no significant difference in the PSA progression-free survival between the ≥75-year-old and <75-year-old groups. Patients in the ≥75-year-old group, particularly those whose doses were not reduced, experienced several Grade 3 to 4 adverse effects. Ten patients discontinued treatment owing to adverse effects and systemic worsening.
Conclusions: To use cabazitaxel effectively, starting administration as early as possible before disease progression is important, and even if Grade 3 to 4 leukopenia and neutropenia are observed during the first course, it is important to carefully maintain the dose. Even when treating elderly patients, reducing the dose does not reduce therapeutic efficacy. However, because this cohort experienced several ≥ Grade 3 adverse effects, a great deal of caution is required.
Keywords: AE, adverse event; CRPC, castrate-resistant prostate cancer; Cabazitaxel; Castration-resistant prostate cancer; FN, febrile neutropenia; GS, Gleason Score; HR, hazard ratio; Leukopenia; NLR, neutrophil/lymphocyte ratio; Neutropenia; OS, overall survival; PS, performance status; PSA, prostate-specific antigen; PSA-PFS, PSA progression-free survival; Safety; WBC, white blood cell; mCRPC, metastatic castrate-resistant prostate cancer.
© 2019 Asian Pacific Prostate Society, Published by Elsevier Korea LLC.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Mukherji D., Omlin A., Pezaro C., Shamseddine A., de Bono J. Metastatic castration-resistant prostate cancer (CRPC): preclinical and clinical evidence for the sequential use of novel therapeutics. Cancer Metastasis Rev. 2014;33(2-3):555–566. - PubMed
-
- Fitzpatrick J.M., Bellmunt J., Fizazi K., Heidenreich A., Sternberg C.N., Tombal B. Optimal management of metastatic castration-resistant prostate cancer: highlights from a European Expert Consensus Panel. Eur J Cancer. 2014;50(9):1617–1627. - PubMed
-
- Chi K., Hotte S.J., Joshua A.M., North S., Wyatt A.W., Collins L.L. Treatment of mCRPC in the AR-axis-targeted therapy-resistant state. Ann Oncol. 2015;26(10):2044–2056. - PubMed
-
- Meisel A., von Felten S., Vogt D.R., Liewen H., de Wit R., de Bono J. Severe neutropenia during cabazitaxel treatment is associated with survival benefit in men with metastatic castration-resistant prostate cancer (mCRPC): A post-hoc analysis of the TROPIC phase III trial. Eur J Cancer. 2016;56:93–100. - PubMed
-
- Miyake H., Sugiyama T., Aki R., Matsushita Y., Tamura K., Motoyama D. No significant impact of prior treatment profile with docetaxel on the efficacy of cabazitaxel in Japanese patients with metastatic castration-resistant prostate cancer. Med Oncol. 2017;34(8):141. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous