

Gamma Knife Radiosurgery for Uveal Melanoma: A Retrospective Review of Clinical Complications in a Tertiary Referral Center
- PMID: 32258019
- PMCID: PMC7109381
- DOI: 10.1159/000501971
Gamma Knife Radiosurgery for Uveal Melanoma: A Retrospective Review of Clinical Complications in a Tertiary Referral Center
Abstract
Introduction: Gamma knife radiosurgery (GKR) has shown promising results in the treatment of intraocular uveal melanoma (UM) in terms of local tumor control. However, GKR is not free from potentially sight-threatening side effects, including cataract, dry eye disease, vitreous hemorrhage, radiation retinopathy (RR), radiation maculopathy (RM), optic neuropathy, and neovascular glaucoma. The aim of this paper is to report our 20-year experience in UM management with GKR focusing on the rate of clinical treatment-induced complications.
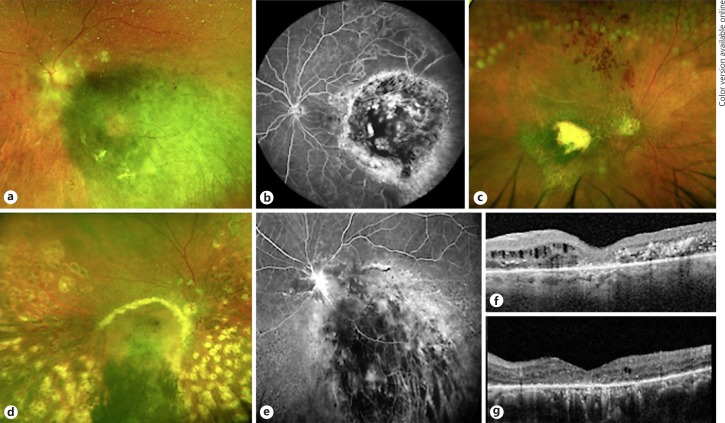
Methods: Single-center, retrospective, observational study, including all patients with UM treated at the Ocular Oncology and Uveitis Service, in the Department of Ophthalmology of the San Raffaele Scientific Institute, Milan from September 1993 to September 2018. Clinical charts comprised complete ophthalmological examination with measurement of best-corrected visual acuity, slit-lamp biomicroscopy, intraocular pressure measurement, gonioscopy, and indirect ophthalmoscopy at each visit. B-scan ultrasound (Aviso S, 10 MHz probe; Paris, France), optical coherence tomography (Heidelberg Spectralis; Heidelberg Engineering, Heidelberg, Germany), retinography, and fundus fluorescein angiography (standard or ultra-widefield [UWF; California, Optos, Dunfermline, Scotland, UK]) were performed aiding in the diagnosis of complications.
Results: Overall, 194 patients (100 males, 51.6%) were reviewed. The median age at the time of the treatment was 65 years (range 27-89) and all participants were Caucasian. In 185 eyes (95.4%), the tumor was primarily located at the choroid. The median follow-up was 57.6 months; radiation-induced complications were found in 145 eyes (74.7%). Radiation-induced cataract and RR were the most frequent events, with a relative incidence of 41.2 and 34.5%, respectively, followed by neovascular glaucoma (27.3%), optic neuropathy (18.6%), RM (11.4%), vitreous hemorrhage (14.4%), phthisis bulbi (7.7%), hyphema (0.5%), and corneal melting (0.5%). The shorter onset of side effects involved the optic nerve (median 14.9 months) and the macula (median 13.7 months).
Conclusion: Despite modern and advanced strategies introduced to limit GKR side effects, cataract and RR still represent a serious limitation of this treatment. Incidence of RR was higher in our cohort compared to other reports, probably due to increased diagnosis rate permitted by UWF retinal imaging.
Keywords: Choroidal melanoma; Gamma knife radiosurgery; Radiation retinopathy; Ultra-widefield imaging.
Copyright © 2019 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no competing interest in publishing the present work.
Figures

References
-
- Singh AD, Bergman L, Seregard S. Uveal melanoma: epidemiologic aspects. Ophthalmol Clin North Am. 2005 Mar;18((1)):75–84. - PubMed
-
- Teikari JM, Raivio I. Incidence of choroidal malignant melanoma in Finland in the years 1973-1980. Acta Ophthalmol (Copenh) 1985 Dec;63((6)):661–5. - PubMed
-
- Isager P, Østerlind A, Engholm G, Heegaard S, Lindegaard J, Overgaard J, et al. Uveal and conjunctival malignant melanoma in Denmark, 1943-97: incidence and validation study. Ophthalmic Epidemiol. 2005 Aug;12((4)):223–32. - PubMed
LinkOut - more resources
Full Text Sources
