

Biomechanical Analysis of Various Reconstructive Methods for the Mandibular Body and Ramus Defect Using a Free Vascularized Fibula Flap
- PMID: 32258153
- PMCID: PMC7094202
- DOI: 10.1155/2020/8797493
Biomechanical Analysis of Various Reconstructive Methods for the Mandibular Body and Ramus Defect Using a Free Vascularized Fibula Flap
Abstract
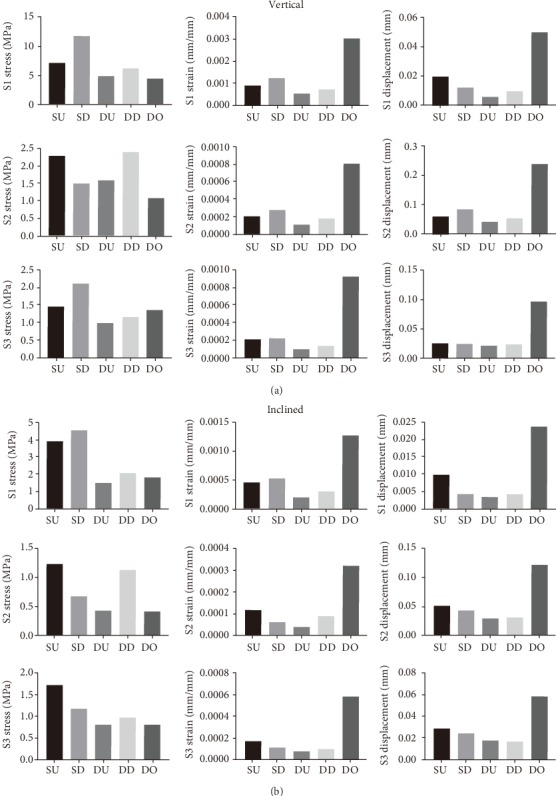
Several different methods exist for reconstructing the mandibular body and ramus defect with the use of a free vascularized fibula flap, but none have adequately addressed the long-term mechanical stability and osseointegration. The aim of this study is to compare the biomechanics of different surgical methods and to investigate the best approach for reconstructing the mandibular body and ramus defect. Five finite element models based on different reconstructive methods were simulated. Stress, strain, and displacement of connective bone sections were calculated for five models and compared. The models were printed using a 3D printer, and stiffness was measured using an electromechanical universal testing machine. The postoperative follow-up cone beam computed tomography (CBCT) was taken at different time points to analyze bone mineral density of connective bone sections. The results showed that the "double up" (DU) model was the most efficient for reconstructing a mandibular body and ramus defect by comparing the mechanical distribution of three sections under vertical and inclined loading conditions of 100 N. The stiffness detection showed that stiffness in the DU and "double down" (DD) models was higher compared with the "single up" (SU), "single down" (SD), and "distraction osteogenesis" (DO) models. We used the DU model for the surgery, and postoperative follow-up CBCT showed that bone mineral density of each fibular connective section increased gradually with time, plateauing at 12 weeks. We conclude that a free vascularized fibula flap of the DU type was the best approach for the reconstruction of the mandibular body and ramus defect. Preoperative finite element analysis and stiffness testing were shown to be very useful for maxillofacial reconstruction.
Copyright © 2020 Xian Li et al.
Conflict of interest statement
None of the authors has a proprietary or financial interest in any product mentioned.
Figures








References
-
- Vittayakittipong P., Jarudejkajon J., Kirirat P., Chaijaroonkhanarak W., Chaisiwamongkol K. Feasibility of the vascularized fibula bone graft for reconstruction of the mandible: a cadaveric study. International Journal of Oral and Maxillofacial Surgery. 2016;45(8):960–963. doi: 10.1016/j.ijom.2015.11.016. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
