

Magnification endoscopy in combination with acetic acid enhancement and narrow-band imaging for the accurate diagnosis of colonic neoplasms
- PMID: 32258370
- PMCID: PMC7089791
- DOI: 10.1055/a-1068-2056
Magnification endoscopy in combination with acetic acid enhancement and narrow-band imaging for the accurate diagnosis of colonic neoplasms
Abstract
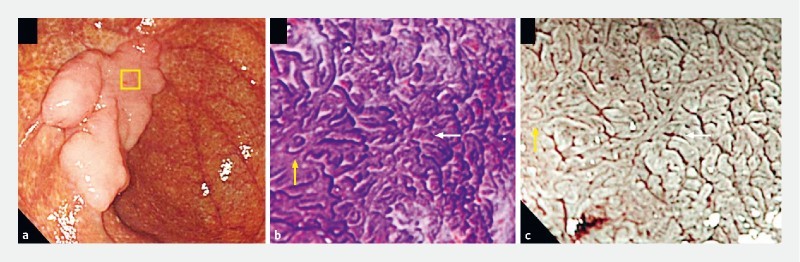
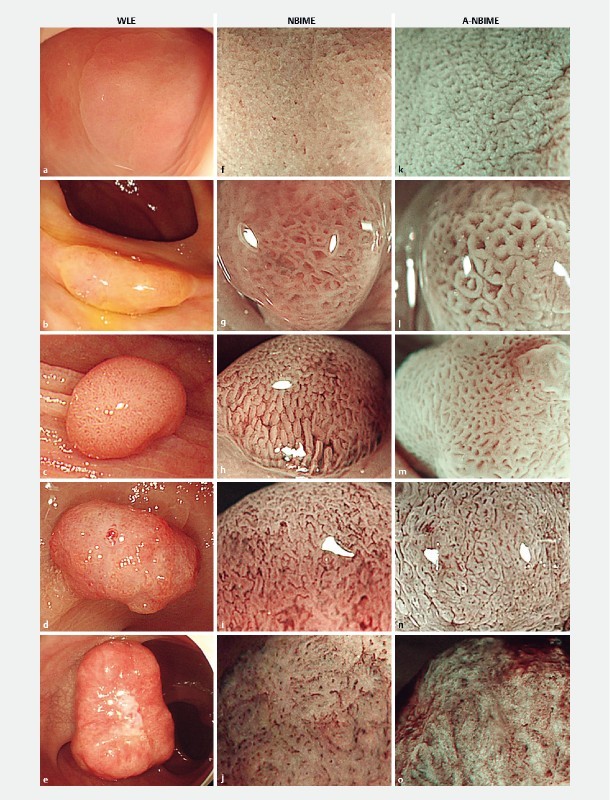
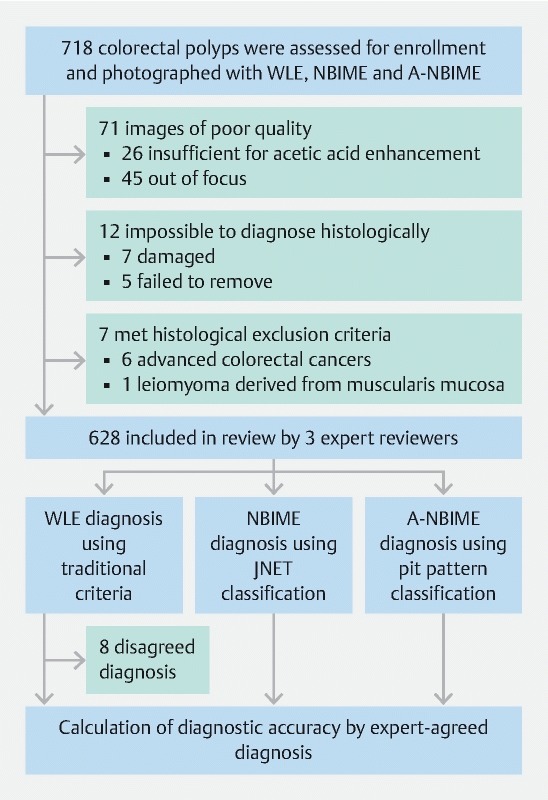
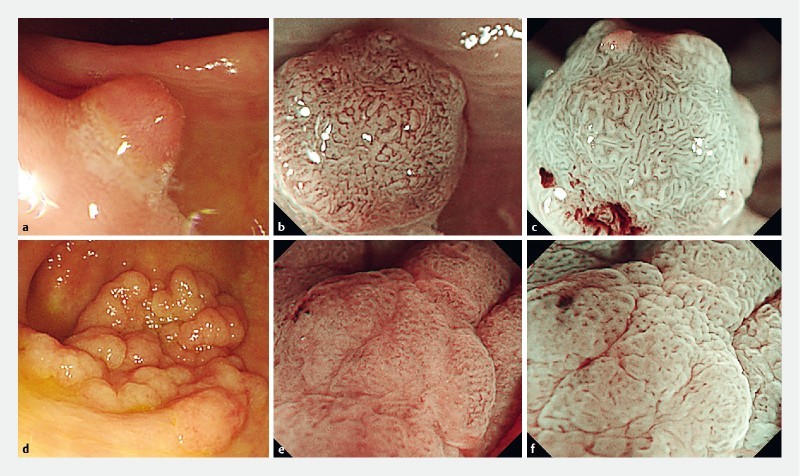
Background and study aims Magnification endoscopy with narrow-band imaging (NBIME) and NBIME with acetic acid enhancement (A-NBIME) enable visualization of the vascular and microstructural patterns of colorectal polyp. We compared the diagnostic accuracy and reproducibility of white light endoscopy (WLE), NBIME, and A-NBIME for predictive histologic diagnosis. Patients and methods Consecutive colorectal polyps (N = 628; 38 hyperplasias, 488 adenomas, 72 M-SM1 cancers, and 30 SM2 cancers) were photographed with WLE, NBIME, and A-NBIME. Endoscopic images were independently reviewed by three experts, according to the traditional criteria for WLE, the Japan NBI Expert Team classification for NBIME, and pit pattern classification for A-NBIME to compare diagnostic accuracy and interobserver diagnostic agreement among modalities. Results The specificity (95 % confidence interval) of hyperplasia and SM2 cancer with WLE were 98.2 % (96.8 %-99.1%) and 99.4 % (98.5 %-99.9 %), respectively, showing high accuracy for endoscopic resection without magnifying observation. Diagnostic accuracy of WLE, NBIME, and A-NBIME was 80.8 % (77.4 %-83.8 %), 79.3 % (75.9 %-82.4 %), and 86.1 % (83.2 %-88.7 %), respectively, showing the highest accuracy for A-NBIME among modalities ( P < .05). NBIME showed a lower PPV for M-SM1 cancer ( P < .05), as with WLE ( P = .08) compared to A-NBIME. Fleiss's kappa values for WLE, NBIME, and A-NBIME diagnosis were 0.43 (0.39 - 0.46), 0.52 (0.49 - 0.56) and 0.65 (0.62 - 0.69), respectively, showing insufficient reproducibility of WLE and superiority of A-NBIME among modalities. Conclusion WLE showed high accuracy for endoscopic resection of colorectal polyps in expert diagnosis. NBIME demonstrated a higher diagnostic reproducibility than WLE. A-NBIME showed possible superiority among modalities in both diagnostic accuracy and reproducibility.
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Diagnostic accuracy of magnification endoscopy with acetic acid enhancement and narrow-band imaging in gastric mucosal neoplasms.Endoscopy. 2016 Jan;48(1):16-25. doi: 10.1055/s-0034-1392542. Epub 2015 Jul 9. Endoscopy. 2016. PMID: 26158242 Clinical Trial.
-
Magnification endoscopy with acetic acid enhancement and a narrow-band imaging system for pit pattern diagnosis of colorectal neoplasms.J Clin Gastroenterol. 2015 Apr;49(4):306-12. doi: 10.1097/MCG.0000000000000148. J Clin Gastroenterol. 2015. PMID: 24804989
-
The value of three narrow-band imaging model in the diagnosis of small colorectal polyps.Sci Rep. 2020 Dec 16;10(1):22032. doi: 10.1038/s41598-020-78708-1. Sci Rep. 2020. PMID: 33328496 Free PMC article.
-
Depth diagnosis of early colorectal cancer: Magnifying chromoendoscopy or image enhanced endoscopy with magnification?Dig Endosc. 2022 Jan;34(2):265-273. doi: 10.1111/den.14087. Epub 2021 Aug 9. Dig Endosc. 2022. PMID: 34289171 Review.
-
Additional chromoendoscopy for colorectal lesions initially diagnosed with low confidence by magnifying narrow-band imaging: Can it improve diagnostic accuracy?Dig Endosc. 2018 Apr;30 Suppl 1:45-50. doi: 10.1111/den.13055. Dig Endosc. 2018. PMID: 29658652 Review.
Cited by
-
Can Ultrasound Elastography Discriminate between Rectal Adenoma and Cancer? A Systematic Review.Cancers (Basel). 2021 Aug 18;13(16):4158. doi: 10.3390/cancers13164158. Cancers (Basel). 2021. PMID: 34439313 Free PMC article. Review.
-
Diagnostic efficacy of the Japan Narrow-band-imaging Expert Team and Pit pattern classifications for colorectal lesions: A meta-analysis.World J Gastroenterol. 2020 Oct 28;26(40):6279-6294. doi: 10.3748/wjg.v26.i40.6279. World J Gastroenterol. 2020. PMID: 33177800 Free PMC article.
References
-
- IARC . Cancer Today. http://gco.iarc.fr/today/fact-sheets-cancers http://gco.iarc.fr/today/fact-sheets-cancers
-
- Winawer S J, Zauber A G, Ho M N et al.Prevention of colorectal cancer by colonoscopic polypectomy: The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981. - PubMed
-
- Kudo S, Tamura S, Nakajima T et al.Diagnosis of colorectal tumorous lesions by magnifying endoscopy. Gastrointest Endosc. 1996;44:8–14. - PubMed
-
- Fujii T, Hasegawa R T, Saitoh Y et al.Chromoscopy during colonoscopy. Endoscopy. 2001;33:1036–1041. - PubMed
-
- Tanaka S, Kaltenbach T, Chayama K et al.High magnification colonoscopy (with videos) Gastrointest Endosc. 2006;64:604–613. - PubMed
LinkOut - more resources
Full Text Sources