

Streptococcus Pneumoniae-associated Thrombotic Microangiopathy in an Immunosuppressed Adult
- PMID: 32258416
- PMCID: PMC7101476
- DOI: 10.1515/med-2020-0030
Streptococcus Pneumoniae-associated Thrombotic Microangiopathy in an Immunosuppressed Adult
Abstract
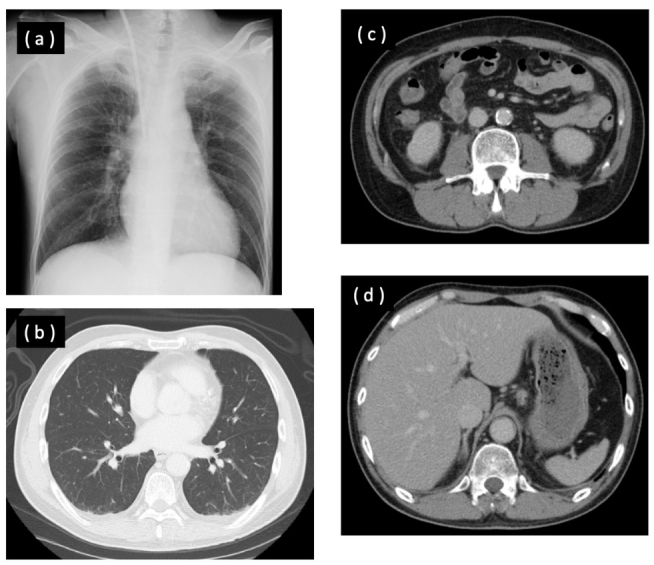
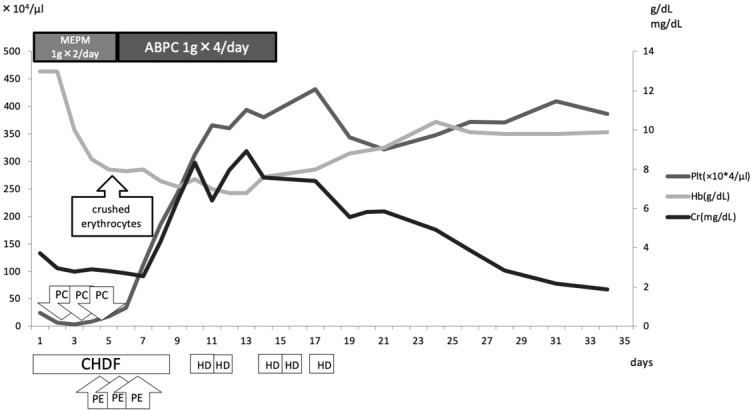
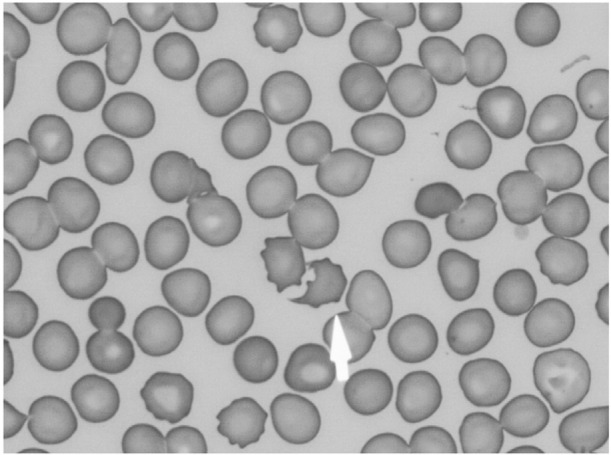
A 62-year-old male who was receiving prednisolone and methotrexate for scleroderma and rheumatoid arthritis complained of diarrhea and vomiting, and was transferred to our hospital for detailed examination and treatment of renal dysfunction and thrombocytopenia. Hemolytic anemia and crushed erythrocytes were found during the patient's course; therefore, we suspected thrombotic microangiopathy (TMA). His ADAMTS13 activity was 60.3% and his ADAMTS13 inhibitor was under 0.5. In addition, his blood culture was positive for Streptococcus pneumoniae, and we finally diagnosed Streptococcus pneumoniae-associated TMA (pTMA). The patient was treated with antibiotics and hemodialysis. The patient recovered and was discharged on the 45th hospital day. Adult pTMA cases are remarkably rare. We herein report a successfully treated adult case of pTMA.
Keywords: Antibiotics; Hemolytic uremic syndrome; Infection; Plasma exchange.
© 2020 Yumi Ichikawa et al., published by De Gruyter.
Conflict of interest statement
Conflict of interest Conflict of interest statement: Authors state no conflict of interest
Figures
References
-
- Goodship T. H. J., Cook H. T., Fakhouri F., Fervenza F. C., Frémeaux-Bacchi V., Kavanagh D.. Atypical hemolytic uremic syndrome and C3 glomerulopathy: conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int. 2017;91(3):539–551. doi: 10.1016/j.kint.2016.10.005. et al. - DOI - PubMed
LinkOut - more resources
Full Text Sources