

Peri-transplant renal dysfunction in patients with non-alcoholic steatohepatitis undergoing liver transplantation
- PMID: 32258522
- PMCID: PMC7063492
- DOI: 10.21037/tgh.2019.10.11
Peri-transplant renal dysfunction in patients with non-alcoholic steatohepatitis undergoing liver transplantation
Abstract
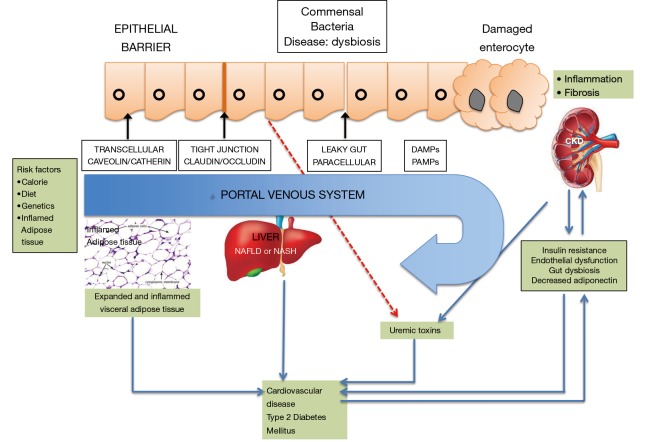
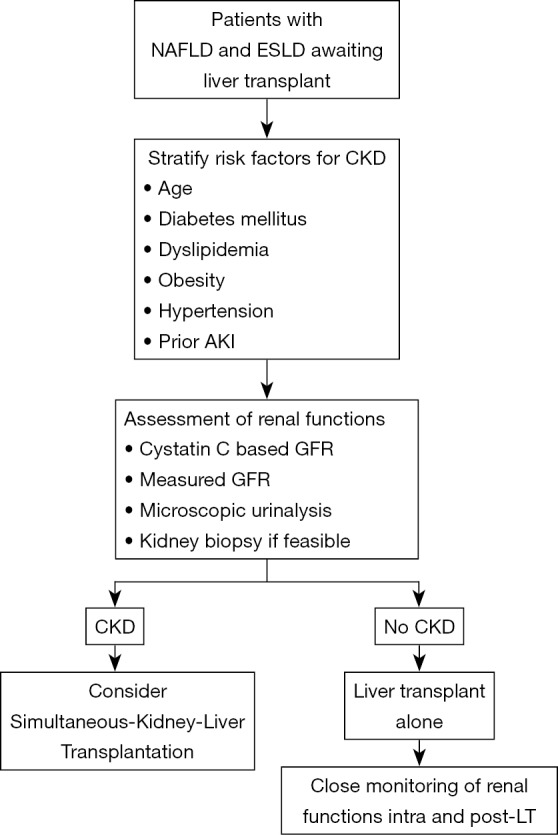
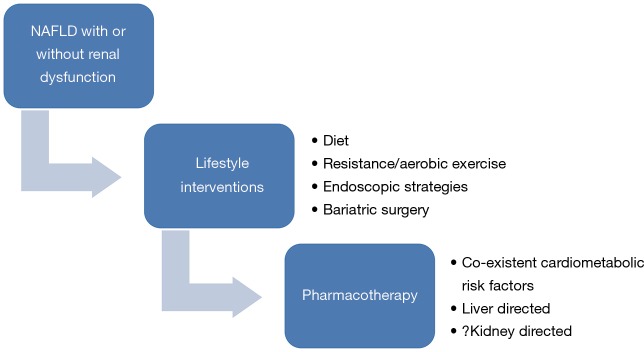
Non-alcoholic fatty liver disease (NAFLD) is currently the most common etiology of chronic liver disease (CLD) caused by an accumulation of fat in the liver and globally is the leading indication of liver transplantation. Emerging data has recognized an increased association of NAFLD with risk of other metabolic liver diseases like type 2 diabetes mellitus, chronic kidney disease (CKD) and cardiovascular diseases. Pathophysiologically, NAFLD patients have a state of low-grade systemic inflammation, insulin resistance and atherogenic dyslipidemia which causes renal dysfunction. Patients with NAFLD cirrhosis awaiting liver transplant (LT) face unique challenges and have a significantly higher requirement of simultaneous-liver-kidney transplant as compared to other etiologies. Further, NAFLD not only recurs but also occurs as a de novo manifestation post-LT. There is also a significantly higher risk of waiting list stagnation and dropouts due to burdensome cardiometabolic disorders in NAFLD patients. The current review aims to understand the prevalence and pathogenetic basis of renal dysfunction in NAFLD. Additionally, the review describes the choice of immunosuppression protocols and use of intraoperative renal replacement therapy in context of intra and post-operative renal dysfunction in NAFLD patients. Prospective controlled trials focusing on NAFLD and development of CKD are needed to assess the existence of a causal and/or a bidirectional relationship between NAFLD and CKD.
Keywords: Non-alcoholic fatty liver disease (NAFLD); cardio-metabolic disorders; chronic kidney disease (CKD); diabetes; dyslipidemia; gut dysbiosis; hypertension; obesity.
2020 Translational Gastroenterology and Hepatology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Nonalcoholic Fatty Liver Disease: Key Considerations Before and After Liver Transplantation.Dig Dis Sci. 2016 May;61(5):1406-16. doi: 10.1007/s10620-016-4035-3. Epub 2016 Jan 27. Dig Dis Sci. 2016. PMID: 26815171 Free PMC article. Review.
-
Non-Alcoholic Fatty Liver Disease: The Emerging Burden in Cardiometabolic and Renal Diseases.Diabetes Metab J. 2017 Dec;41(6):430-437. doi: 10.4093/dmj.2017.41.6.430. Epub 2017 Nov 17. Diabetes Metab J. 2017. PMID: 29199410 Free PMC article. Review.
-
NAFLD and liver transplantation: Disease burden, current management and future challenges.JHEP Rep. 2020 Oct 9;2(6):100192. doi: 10.1016/j.jhepr.2020.100192. eCollection 2020 Dec. JHEP Rep. 2020. PMID: 33163950 Free PMC article. Review.
-
Peri-transplant management of nonalcoholic fatty liver disease in liver transplant candidates .Transl Gastroenterol Hepatol. 2020 Jan 5;5:10. doi: 10.21037/tgh.2019.09.09. eCollection 2020. Transl Gastroenterol Hepatol. 2020. PMID: 32190778 Free PMC article. Review.
-
A brief review on the rising incidence of chronic kidney diseases and non-alcoholic fatty liver disease.Physiol Int. 2019 Dec 1;106(4):305-310. Physiol Int. 2019. PMID: 31906711 Review.
Cited by
-
Liver transplantation in patients with non-alcoholic steatohepatitis and alcohol-related liver disease: the dust is yet to settle.Transl Gastroenterol Hepatol. 2022 Jul 25;7:23. doi: 10.21037/tgh-2020-15. eCollection 2022. Transl Gastroenterol Hepatol. 2022. PMID: 35892055 Free PMC article. No abstract available.
References
-
- Guzman G, Brunt EM, Petrovic LM, et al. Does nonalcoholic fatty liver disease predispose patients to hepatocellular carcinoma in the absence of cirrhosis? Arch Pathol Lab Med 2008;132:1761-6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources