

Recognition of chronic hypoxia and pre-existing foetal injury on the cardiotocograph (CTG): Urgent need to think beyond the guidelines
- PMID: 32258602
- PMCID: PMC6806963
- DOI: 10.1016/j.pbj.2017.01.004
Recognition of chronic hypoxia and pre-existing foetal injury on the cardiotocograph (CTG): Urgent need to think beyond the guidelines
Abstract
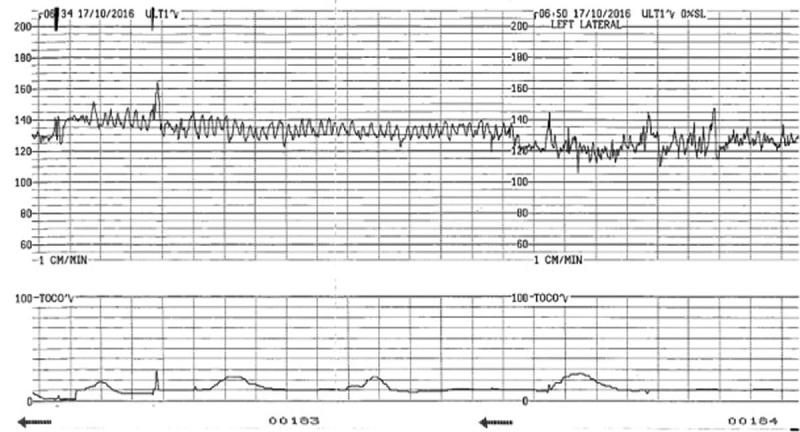
Chronic utero-placental insufficiency may result in progressive hypoxia culminating in fetal decompensation and acidosis and this is termed 'chronic' or 'long-standing' hypoxia. It is essential to recognise the features of chronic hypoxia on the CTG trace so as to institute timely and appropriate action. The current guidelines may not capture a fetus who starts labour already compromised or limited in its ability to compensate for hypoxic or mechanical stresses during labour. The aim of this short review is to explore the CTG features that allow the clinician to recognise a fetus who may present with an antenatal insult such as chronic hypoxia, anaemia, infection, fetal arrhythmias and preexisting non-hypoxic brain injury.
Keywords: CTG monitoring; Cardiotocography; Chronic hypoxia; Fetal anaemia; Fetal stroke.
Copyright 2017 PBJ-Associação Porto Biomedical/Porto Biomedical Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





Similar articles
-
International expert consensus statement on physiological interpretation of cardiotocograph (CTG): First revision (2024).Eur J Obstet Gynecol Reprod Biol. 2024 Nov;302:346-355. doi: 10.1016/j.ejogrb.2024.09.034. Epub 2024 Oct 2. Eur J Obstet Gynecol Reprod Biol. 2024. PMID: 39378709
-
Types of intrapartum hypoxia on the cardiotocograph (CTG): do they have any relationship with the type of brain injury in the MRI scan in term babies?J Obstet Gynaecol. 2020 Jul;40(5):688-693. doi: 10.1080/01443615.2019.1652576. Epub 2019 Oct 15. J Obstet Gynaecol. 2020. PMID: 31612740
-
Prevention of birth asphyxia: responding appropriately to cardiotocograph (CTG) traces.Best Pract Res Clin Obstet Gynaecol. 2007 Aug;21(4):609-24. doi: 10.1016/j.bpobgyn.2007.02.008. Epub 2007 Mar 30. Best Pract Res Clin Obstet Gynaecol. 2007. PMID: 17400026 Review.
-
Continuous cardiotocography during labour: Analysis, classification and management.Best Pract Res Clin Obstet Gynaecol. 2016 Jan;30:33-47. doi: 10.1016/j.bpobgyn.2015.03.022. Epub 2015 Jun 25. Best Pract Res Clin Obstet Gynaecol. 2016. PMID: 26165747 Review.
-
The CTG and the timing and mechanism of fetal neurological injuries.Best Pract Res Clin Obstet Gynaecol. 2004 Jun;18(3):437-56. doi: 10.1016/j.bpobgyn.2004.03.001. Best Pract Res Clin Obstet Gynaecol. 2004. PMID: 15183138 Review.
Cited by
-
Severe Neonatal Anemia Due to Spontaneous Massive Fetomaternal Hemorrhage at Term: An Illustrative Case with Suspected Antenatal Diagnosis and Brief Review of Current Knowledge.Medicina (Kaunas). 2021 Nov 23;57(12):1285. doi: 10.3390/medicina57121285. Medicina (Kaunas). 2021. PMID: 34946230 Free PMC article. Review.
-
Relative uteroplacental insufficiency of labor.Acta Obstet Gynecol Scand. 2024 Oct;103(10):1910-1918. doi: 10.1111/aogs.14937. Epub 2024 Aug 6. Acta Obstet Gynecol Scand. 2024. PMID: 39107951 Free PMC article. Review.
-
Accuracy of a Noninvasive, Wearable, Wireless, ECG-Based, Intrapartum Monitoring Tool Against the Conventional Ultrasound-Based CTG.J Obstet Gynaecol India. 2025 Apr;75(Suppl 1):340-347. doi: 10.1007/s13224-024-01998-2. Epub 2024 Aug 31. J Obstet Gynaecol India. 2025. PMID: 40390897
-
Pustular psoriasis of pregnancy: A rare cause of placental insufficiency.Obstet Med. 2024 Dec;17(4):236-239. doi: 10.1177/1753495X221149134. Epub 2023 Jan 10. Obstet Med. 2024. PMID: 39640954 Free PMC article.
-
Abnormal heart rate pattern in fetal anaemia secondary to transient abnormal myelopoeisis in a fetus without trisomy 21: A case report.Case Rep Womens Health. 2023 May 4;38:e00512. doi: 10.1016/j.crwh.2023.e00512. eCollection 2023 Jun. Case Rep Womens Health. 2023. PMID: 37234955 Free PMC article.
References
-
- Ayres-de-Campos D, Spong KY, Chandraharan E. for the FIGO intrapartum fetal monitoring consensus panel. Cardiotocography Int J Gynecol Obstet. 2015;131:13-24. - PubMed
-
- Yanamandra N, Chandraharan E. Saltatory and sinusoidal fetal heart rate (FHR) patterns and significance of FHR ‘overshoots’. Curr Wom Health Rev. 2013;9:1e8.
-
- Nurani R, Chandraharan E, Lowe V, Ugwumadu A, Arulkumaran S. Misidentification of maternal heart rate as fetal on cardiotocography during the second stage of labor: the role of the fetal electrocardiograph. Acta Obstet Gynecol Scan. 2012;91:142832. - PubMed
-
- Gagnon R, Hunse C, Bocking AD. Fetal heart rate patterns in the small-for-gestational-age human fetus. Am J Obstet Gynecol. 1989;161:779-784. - PubMed
-
- Murotsuki J, Bocking AD, Gagnon R. Fetal heart rate patterns in growth-restricted fetal sheep induced by chronic fetal placental embolization. Am J Obstet Gynecol. 1997;176:282-290. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources