

Retinal arterial occlusive vasculitis following intravitreal brolucizumab administration
- PMID: 32258827
- PMCID: PMC7125319
- DOI: 10.1016/j.ajoc.2020.100680
Retinal arterial occlusive vasculitis following intravitreal brolucizumab administration
Abstract
Purpose: To describe retinal arterial occlusion and vasculitis following intravitreal brolucizumab administration in a patient with neovascular age-related macular degeneration (nAMD).
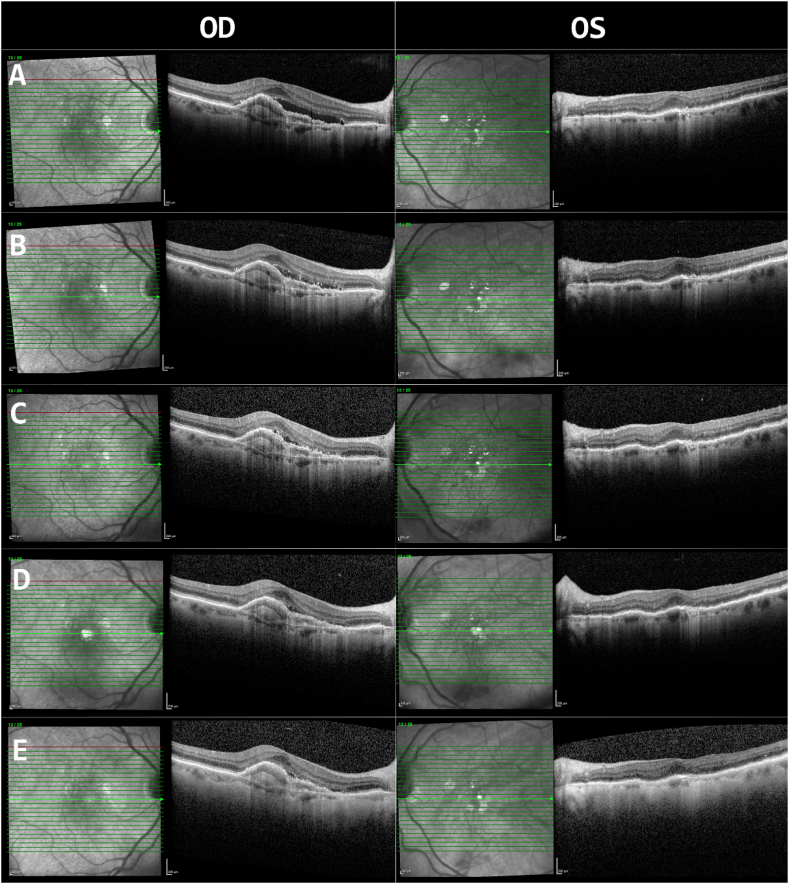
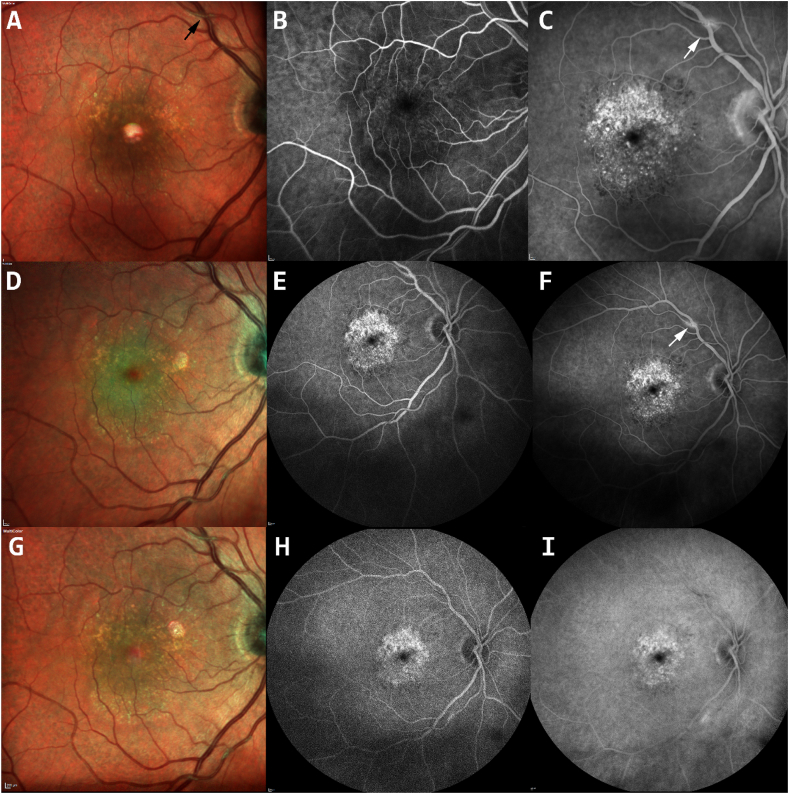
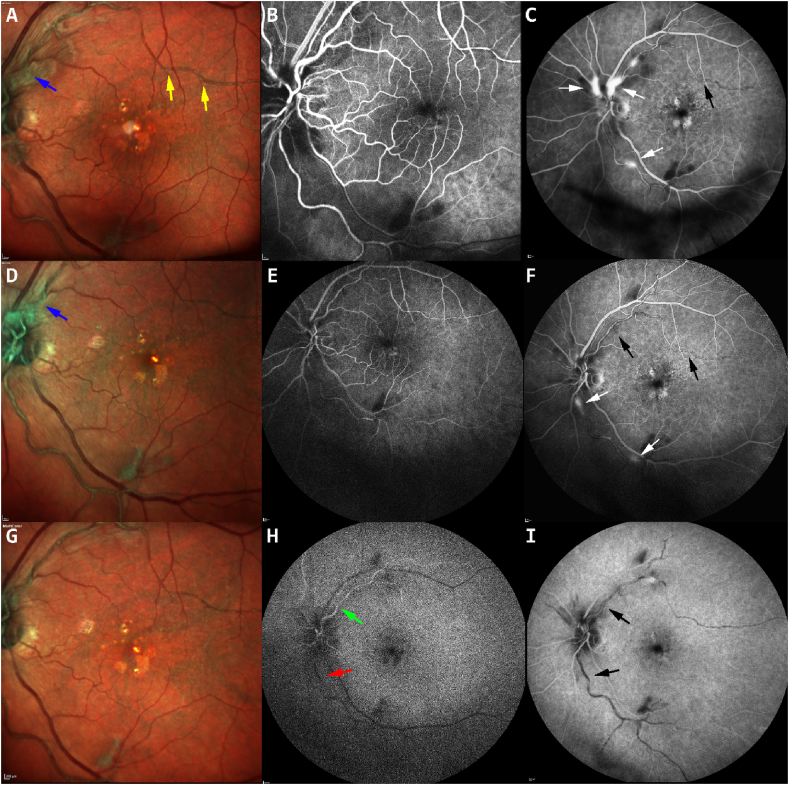
Observation: An 88-year-old Caucasian woman with neovascular age-related macular degeneration (nAMD) complained of painless loss of vision with light sensitivity in both eyes (OU) four weeks after bilateral intravitreal brolucizumab. Upon examination, her visual acuity decreased to 20/40 in the right eye (OD) and 20/50 in the left eye (OS). Examination revealed 0.5+ and 1+ anterior chamber cells in OD and OS, respectively. The patient was treated with 1% prednisolone acetate eyedrops in both eyes, and after several weeks, the anterior chamber cells resolved. However, the patient still reported a decline in visual acuity (VA). Fluorescein angiography (FA) revealed retinal arterial occlusion, vasculitis, and optic nerve inflammation in the left eye. Retinal intra-arterial grayish materials were also detected. Laboratory evaluations were performed for common infectious and inflammatory causes and were normal or negative. A delayed inflammatory reaction to brolucizumab was suspected as the cause of the ocular inflammation and retinal vasculitis. An intravitreal dexamethasone implant was inserted into the left eye to treat the inflammation. One week after the dexamethasone implant, VA improved to 20/40 in OU; FA showed improvement, but residual peri-vascular leakage remained.
Conclusion: Medication-associated uveitis is a rare adverse effect that can lead to vision loss. The index report illustrates a case of intraocular inflammation, retinal arterial vaso-occlusion and vasculitis associated with intravitreal brolucizumab. The delay in developing uveitis suggests that the inflammation is due to a delayed hypersensitivity reaction which can occur several days or weeks after administration of the inciting agent. Recently, several cases of uveitis and vasculitis associated with brolucizumab have been presented and those cases have similar features compared to the index case (1). Therapy with steroids (either intraocular or systemic), after infectious etiologies have been excluded, may be beneficial in halting inflammation and preventing further vision loss.
Keywords: Age-related macular degeneration; Brolucizumab; Intraocular inflammation; Occlusive vasculitis; Retinal vasculitis.
© 2020 The Authors.
Conflict of interest statement
The authors declare that there are no conflicts of interest related to this article.
Figures
References
-
- Dugel P.U. Presented at the 2020 Meeting of the Macula Society, March 19 to 22, San Diego, California. 2017. Expanded week 96 safety outcomes: analysis of pooled data from HAWK & HARRIER studies.
-
- Dugel P.U., Koh A., Ogura Y. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72–84. - PubMed
-
- Nguyen Q.D., Das A., Do D.V. Brolucizumab: evolution through preclinical and clinical studies and the implications for the management of neovascular age-related macular degeneration [published online ahead of print, 2020 Jan 17] Ophthalmology. 2020 S0161-6420(20)30041-5. - PubMed
-
- Veramme J., de Zaeytijd J., Lambert J., Lapeere H. Contact dermatitis in patients undergoing serial intravitreal injections. Contact Dermatitis. 2016;74(1):18–21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
