

Multicenter case series of patients with small-bowel angiodysplasias treated with a small-bowel radiofrequency ablation catheter
- PMID: 32258850
- PMCID: PMC7125393
- DOI: 10.1016/j.vgie.2019.11.014
Multicenter case series of patients with small-bowel angiodysplasias treated with a small-bowel radiofrequency ablation catheter
Abstract
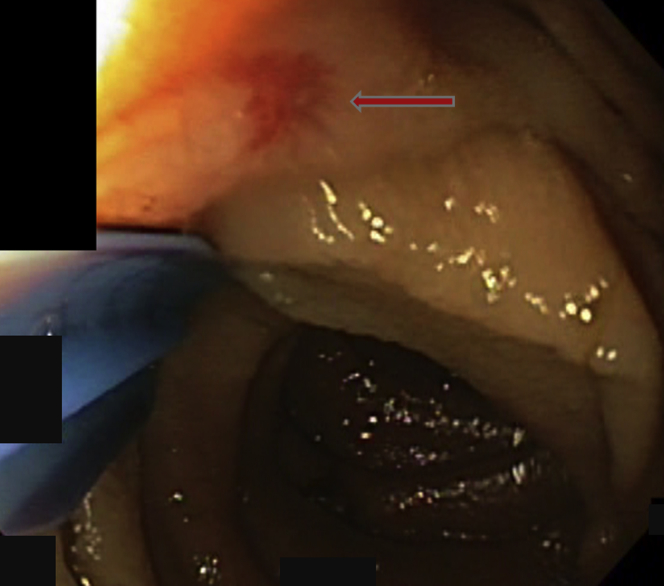
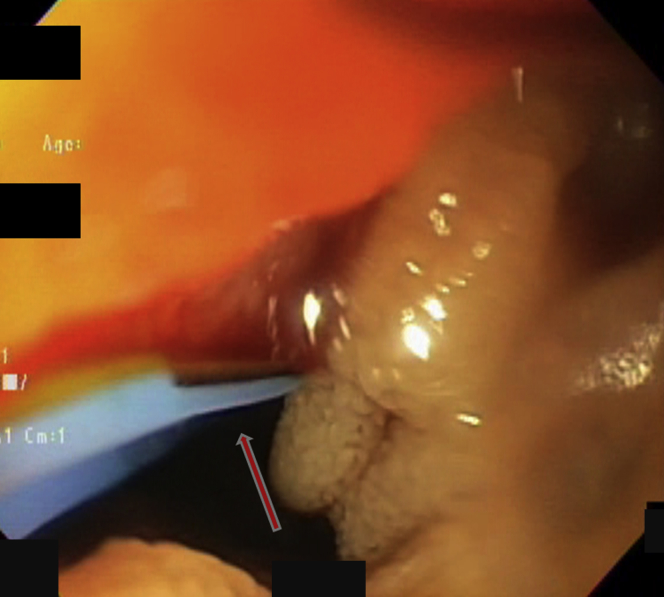
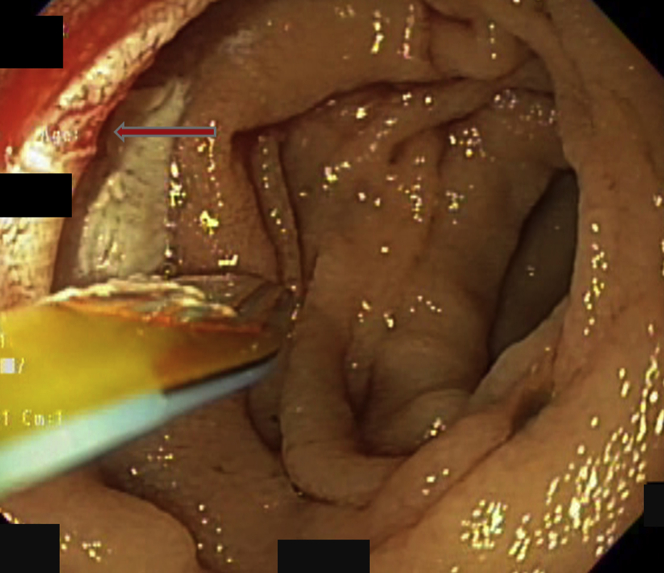
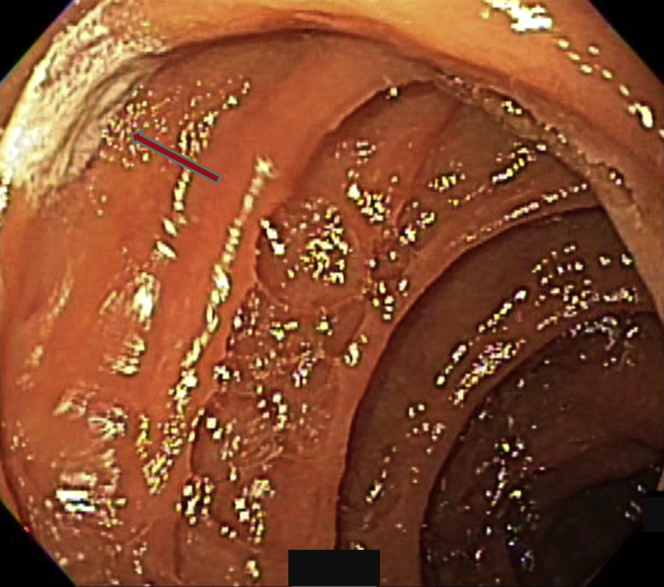
Background and aims: GI angiodysplasia is the most common cause of small-bowel bleeding. Argon plasma coagulation (APC) is preferred for ablation because of its availability, ease of use, and perceived safety, but it has limitations. An instrument capable of repeated use through the enteroscope, which covers more area of intestinal mucosa per treatment with low risk of damage to healthy mucosa, and which improves ablation, is desirable. A series of patients treated with a through-the-scope radiofrequency ablation (RFA) catheter is reported.
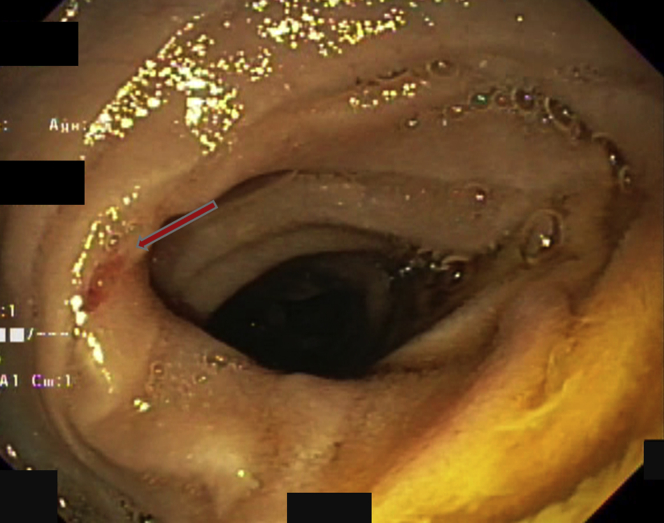
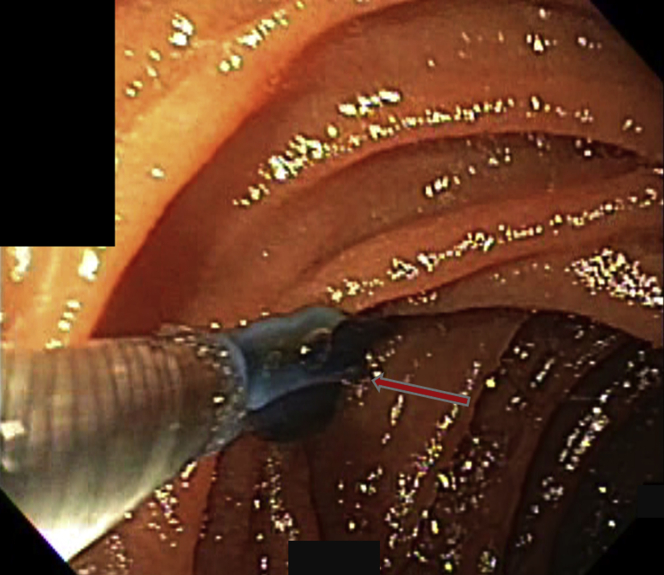
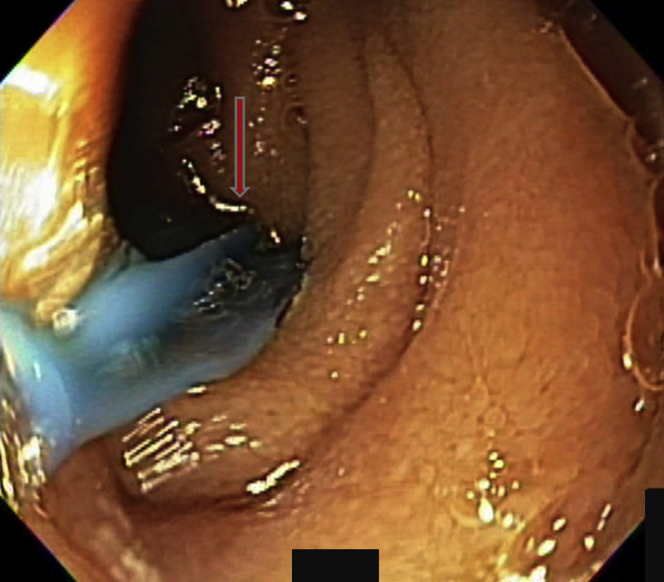
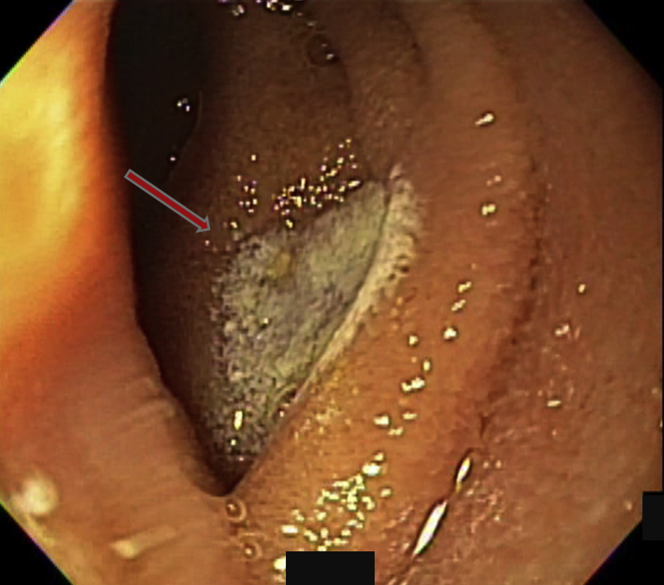
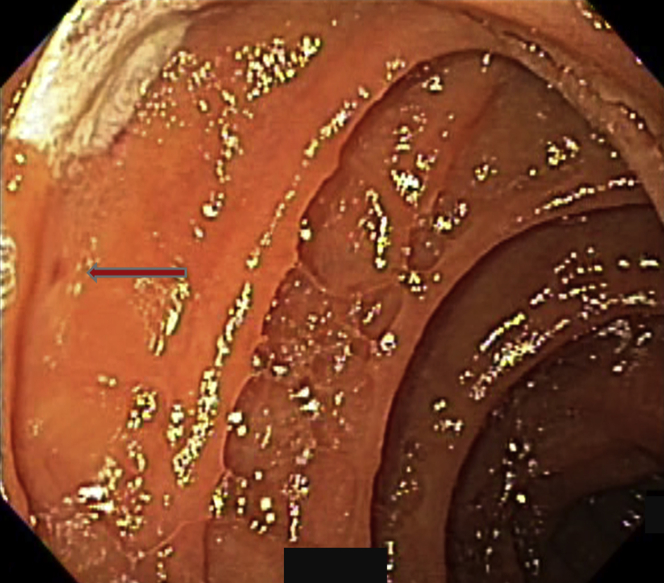
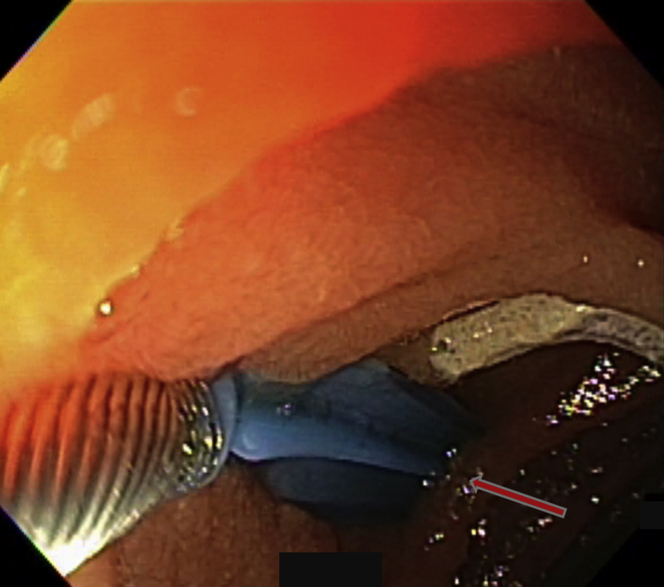
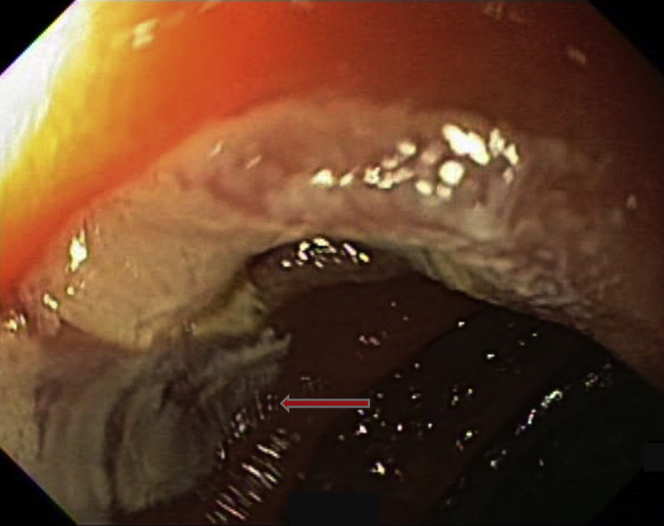
Methods: Patients with a previous diagnosis of small-bowel angiodysplasia (SBA) and ongoing bleeding with melena, hematochezia, or iron-deficiency anemia were eligible for treatment. A small-bowel radiofrequency ablation (SBRFA) catheter was passed through the enteroscope instrument channel. The treatment paddle was pushed against the SBA, achieving coaptive coagulation, and the SBA was treated up to 2 times at standard settings of 10 J/cm2. The patients' demographics, pretreatment and posttreatment hemoglobin levels, time to recurrence of bleeding, and need for more therapy were recorded. This study was approved by the institutional review boards of the respective institutions.
Results: Twenty consecutive patients were treated from March until October 2018 and followed up until March 2019. There were 6 women (average age 68 years, standard deviation ± 11.1), and 14 men (average age 73 years, standard deviation ± 10.4). All had undergone at least 1 previous EGD and colonoscopy; 14 patients (70%) had SBA on video capsule endoscopy, and 14 patients had undergone previous endoscopic treatment of SBA with APC. A median of 23 treatments were applied (range, 2-99). The median follow-up time was 195 days (range, 30-240 days). Four patients, including 3 with a left ventricular assist device (LVAD), had recurrent bleeding between 45 and 210 days after treatment, and 2 patients received repeated blood transfusions. Three of those patients underwent repeated endoscopies, including a push enteroscopy and an upper endoscopy with no treatment, and a repeated enteroscopy with SBA treated with APC, respectively. One patient with LVAD underwent arterial embolization.
Conclusions: In this case series, bleeding recurred in 20% of patients in a follow-up time of ≤240 days. Notably, 3 of the 4 patients who had recurrent bleeding had an LVAD. These rates compare favorably with reported bleeding recurrence after APC of SBA. More studies on the benefits of SBRFA, which may include reduced risk of recurrent bleeding or prolonging the time to recurrent bleeding, resource utilization, and factors associated with bleeding recurrence are needed.
Keywords: APC, argon plasma coagulation; GIAD, GI angiodysplasia; LVAD, left ventricular assist device; RFA, radiofrequency ablation; SBA, small-bowel angiodysplasia; SBRFA, small-bowel radiofrequency ablation.
© 2019 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc.
Figures
References
-
- Sami S.S., Al-Araji S.A., Ragunath K. Review article: gastrointestinal angiodysplasia -pathogenesis, diagnosis and management. Aliment Pharmacol Ther. 2013;39:15–34. - PubMed
-
- Boley S.J., Sammartano R., Adams A. On the nature and etiology of vascular ectasias of the colon. Degenerative lesions of aging. Gastroenterology. 1977;72:650–660. - PubMed
-
- Heer M., Sulser H., Hany A. Angiodysplasia of the colon: an expression of occlusive vascular disease. Hepatogastroenterology. 1987;34:127–131. - PubMed
-
- Junquera F., Saperas E., de Torres I. Increased expression of angiogenic factors in human colonic angiodysplasia. Am J Gastroenterol. 1999;94:1070–1076. - PubMed
-
- Raju G.S., Gerson L., Das A. American Gastroenterological Association (AGA) Institute technical review on obscure gastrointestinal bleeding. Gastroenterology. 2007;133:1697–1717. - PubMed
