

The history of liver surgery: Achievements over the past 50 years
- PMID: 32258975
- PMCID: PMC7105847
- DOI: 10.1002/ags3.12322
The history of liver surgery: Achievements over the past 50 years
Abstract
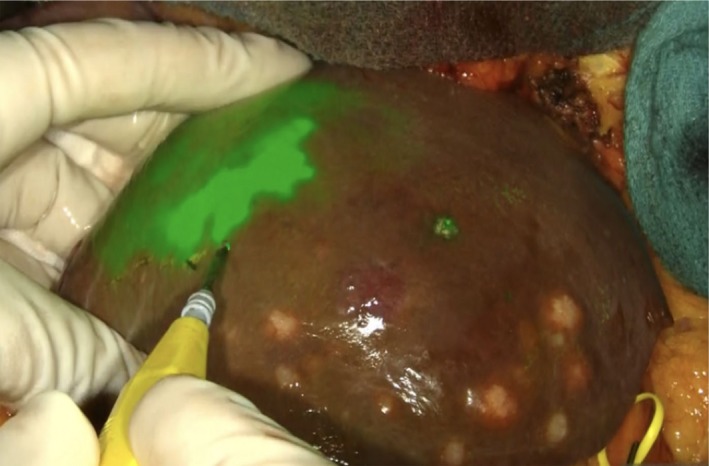
We reviewed the progress made in the field of liver surgery over the past 50 years. The widespread use and improved outcomes of the hepatectomy were, primarily, due to pioneer surgeons who were responsible for technological advances and rapid improvements in the safety of the procedure in the last century. These advances included the hepatic functional evaluation used to determine the safety limit of liver resections, the introduction of intraoperative ultrasonography, and the development of innovative techniques such as portal vein embolization to increase the remnant liver volume. Cadaveric liver transplantation has been attempted since 1963. However, the clinical outcomes only began improving and becoming acceptable in the 1970s-1980s due to refinements in technology and the development of new immunosuppressants. Partial liver transplantation from living donors, which was first attempted in 1988, required further technological innovation and sophisticated perioperative management plans. Moreover, these developments allowed for further overall improvements to take place in the field of liver surgery. Since the turn of the century, advances in computation and imaging technology have made it possible for safer and more elaborate surgeries to be performed. In Japan, preoperative 3-dimensional simulation technology has been covered by health insurance since 2012 and is now widely used. An urgent need for real-time navigation tools will develop in the future. Indocyanine green (ICG) fluorescence imaging was first used in 2007 and has led to the creation of a new surgical concept known as fluorescence navigation surgery. Laparoscopic surgery and robotic surgery have solved the issue of large incisions, which used to be a major drawback of open liver surgery; however, further improvements are required in order to achieve the level of safety and accuracy observed during open liver resection when performing all minimally invasive procedures. In the near future, liver surgery will become more precise and less invasive due to substantial progress including the development of navigation surgery, cancer imaging, and minimally invasive surgery. This overview of the history of liver surgery over the past 50 years may provide useful insights for further innovation in the next 50 years.
© 2020 The Authors. Annals of Gastroenterological Surgery published by John Wiley & Sons Australia, Ltd on behalf of The Japanese Society of Gastroenterology.
Conflict of interest statement
Authors declare no conflict of interests for this article.
Figures





References
-
- Lortat‐Jacob JL. Hepatectomie droite reglee. La presse medicale. 1952;60:N26. - PubMed
-
- Honjo I, Araki C. Total resection of the right lobe of the liver; report of a successful case. J Int Coll Surg. 1955;23:23–8. - PubMed
-
- Lin TY, Chen KM, Liu TK. Total right hepatic lobectomy for primary hepatoma. Surgery. 1960;48:1048–60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
