

Locally Informed Simulation to Predict Hospital Capacity Needs During the COVID-19 Pandemic
- PMID: 32259197
- PMCID: PMC7153364
- DOI: 10.7326/M20-1260
Locally Informed Simulation to Predict Hospital Capacity Needs During the COVID-19 Pandemic
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic challenges hospital leaders to make time-sensitive, critical decisions about clinical operations and resource allocations.
Objective: To estimate the timing of surges in clinical demand and the best- and worst-case scenarios of local COVID-19-induced strain on hospital capacity, and thus inform clinical operations and staffing demands and identify when hospital capacity would be saturated.
Design: Monte Carlo simulation instantiation of a susceptible, infected, removed (SIR) model with a 1-day cycle.
Setting: 3 hospitals in an academic health system.
Patients: All people living in the greater Philadelphia region.
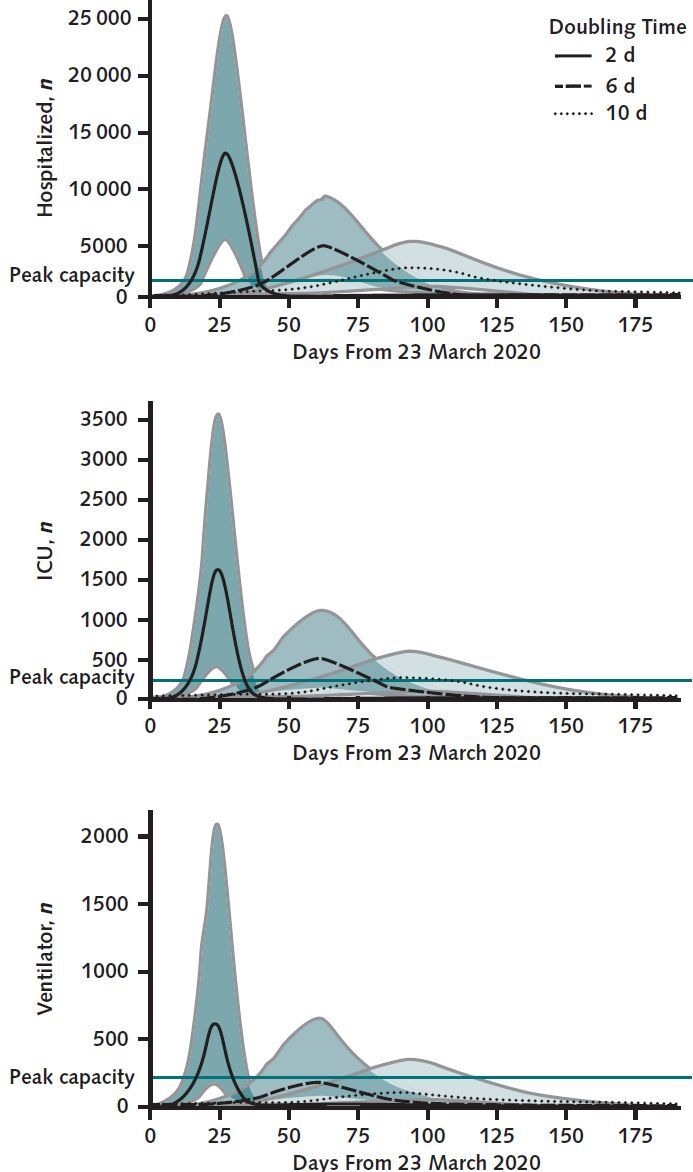
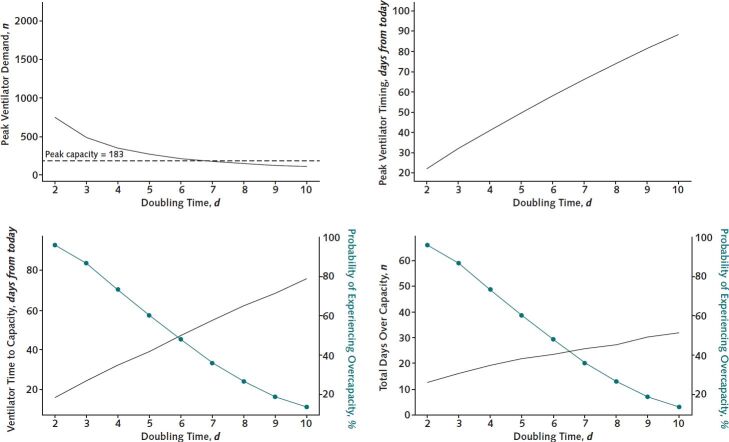
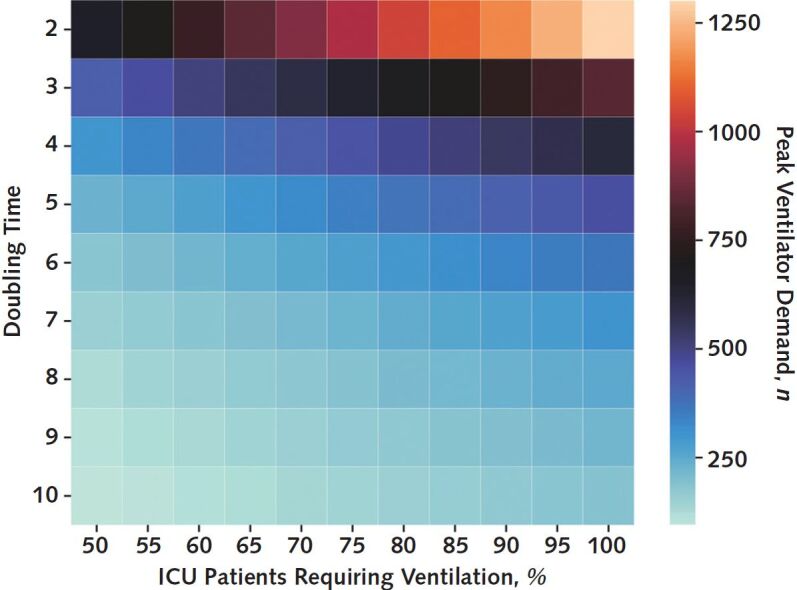
Measurements: The COVID-19 Hospital Impact Model (CHIME) (http://penn-chime.phl.io) SIR model was used to estimate the time from 23 March 2020 until hospital capacity would probably be exceeded, and the intensity of the surge, including for intensive care unit (ICU) beds and ventilators.
Results: Using patients with COVID-19 alone, CHIME estimated that it would be 31 to 53 days before demand exceeds existing hospital capacity. In best- and worst-case scenarios of surges in the number of patients with COVID-19, the needed total capacity for hospital beds would reach 3131 to 12 650 across the 3 hospitals, including 338 to 1608 ICU beds and 118 to 599 ventilators.
Limitations: Model parameters were taken directly or derived from published data across heterogeneous populations and practice environments and from the health system's historical data. CHIME does not incorporate more transition states to model infection severity, social networks to model transmission dynamics, or geographic information to account for spatial patterns of human interaction.
Conclusion: Publicly available and designed for hospital operations leaders, this modeling tool can inform preparations for capacity strain during the early days of a pandemic.
Primary funding source: University of Pennsylvania Health System and the Palliative and Advanced Illness Research Center.
Keywords: COVID-19; Forecasting; Immune system; Intensive care units; Population statistics; Prevention, policy, and public health; Pulmonary diseases; Sensitivity; Upper respiratory tract infections; Ventilators.
Figures
Comment in
-
Locally Informed Simulation to Predict Hospital Capacity Needs During the COVID-19 Pandemic.Ann Intern Med. 2020 Oct 20;173(8):679-680. doi: 10.7326/L20-1061. Ann Intern Med. 2020. PMID: 33075246 No abstract available.
References
-
- Halpern SD. ICU capacity strain and the quality and allocation of critical care. Curr Opin Crit Care. 2011;17:648-57. [PMID: 21986461] doi:10.1097/MCC.0b013e32834c7a53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources