

Association Between Celiac Disease and Mortality Risk in a Swedish Population
- PMID: 32259229
- PMCID: PMC7139272
- DOI: 10.1001/jama.2020.1943
Association Between Celiac Disease and Mortality Risk in a Swedish Population
Abstract
Importance: Celiac disease may be associated with a modest but persistent increased long-term mortality risk. It is uncertain whether this risk has changed in the era of wider diagnosis rates, less severe clinical disease, and more widespread availability of gluten-free food.
Objective: To evaluate the association between celiac disease and mortality risk in a population-based cohort in Sweden.
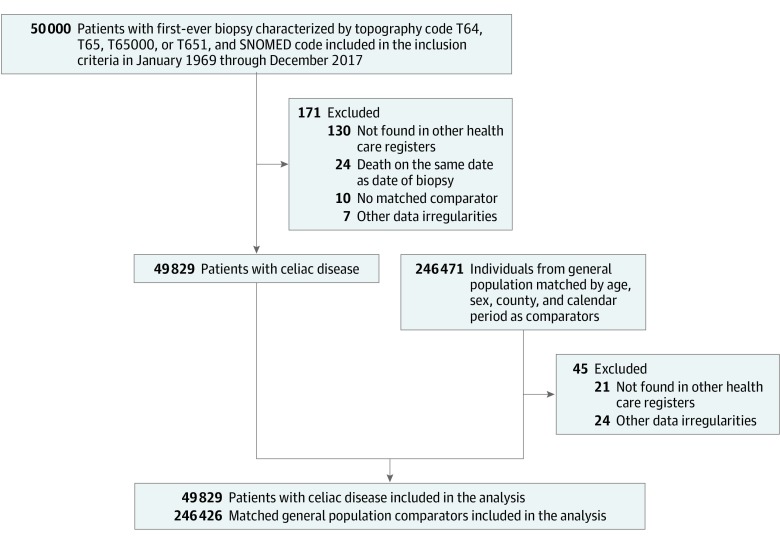
Design, setting, and participants: All individuals in Sweden with celiac disease diagnosed between 1969 and 2017 were identified through the Epidemiology Strengthened by histoPathology Reports in Sweden (ESPRESSO) cohort. Participants (n = 49 829) were observed starting on the day of the biopsy. The final date of follow-up was December 31, 2017.
Exposures: Celiac disease was defined by the presence of small intestinal villus atrophy on histopathology specimens during the years 1969-2017 from Sweden's 28 pathology departments. Each individual was matched with as many as 5 control participants in the general population by age, sex, county, and calendar period.
Main outcomes and measures: The primary outcome was all-cause mortality, and the secondary outcome was cause-specific mortality. Patients with celiac disease were compared with controls using stratified Cox proportional modeling, stratifying by year of diagnosis.
Results: There were 49 829 patients with celiac disease, including 24% who were diagnosed between the years 2010 and 2017. The mean (SD) age at diagnosis was 32.2 (25.2) years and 62.4% were women. During a median follow-up time of 12.5 years, 13.2% (n = 6596) died. Compared with controls (n = 246 426), overall mortality was increased in those with celiac disease (9.7 vs 8.6 deaths per 1000 person-years; absolute difference, 1.2 per 1000 person-years; hazard ratio [HR], 1.21 [95% CI, 1.17-1.25]). The relative increase in mortality risk was present in all age groups and was greatest in those diagnosed in the age range of 18 to 39 years (1.9 vs 1.1 per 1000 person-years; HR, 1.69 [95% CI, 1.47-1.94]; P values for heterogeneity comparing 18-39 years with 40-59 years and with ≥60 years were both <.001). Individuals with celiac disease were at increased risk of death from cardiovascular disease (3.5 vs 3.4 per 1000 person-years; HR, 1.08 [95% CI, 1.02-1.13]), cancer (2.7 vs 2.2 per 1000 person-years; HR, 1.29 [95% CI, 1.22-1.36]), and respiratory disease (0.6 vs 0.5 per 1000 person-years; HR, 1.21 [95% CI, 1.08-1.37]). When compared with controls, the overall mortality risk was greatest in the first year after diagnosis (15.3 vs 6.5 per 1000 person-years; HR, 2.34 [95% CI, 2.14-2.55]) but persisted beyond 10 years after diagnosis (10.5 vs 10.1 per 1000 person-years; HR, 1.15 [95% CI, 1.10-1.20]). The mortality risk was likewise present for patients diagnosed during the years 2010-2017 (7.5 vs 5.5 per 1000 person-years; HR, 1.35 [95% CI, 1.21-1.51]).
Conclusions and relevance: In a Swedish population studied between 1969 and 2017, a diagnosis of celiac disease compared with the general population was associated with a small but statistically significant increased mortality risk.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
