

Hearing with One Ear: Consequences and Treatments for Profound Unilateral Hearing Loss
- PMID: 32260087
- PMCID: PMC7230949
- DOI: 10.3390/jcm9041010
Hearing with One Ear: Consequences and Treatments for Profound Unilateral Hearing Loss
Abstract
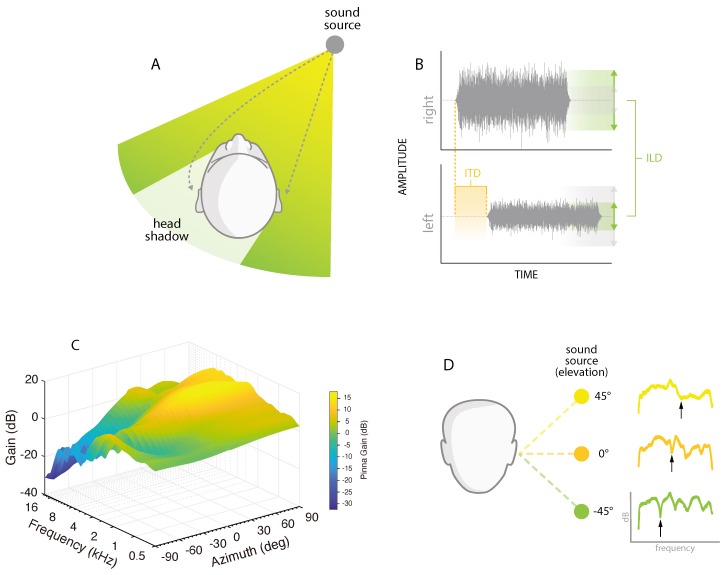
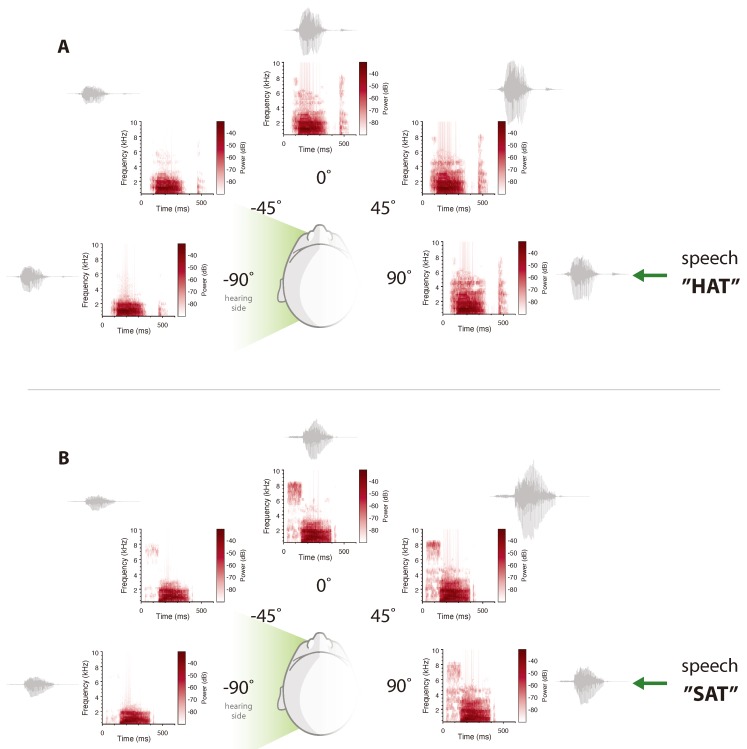
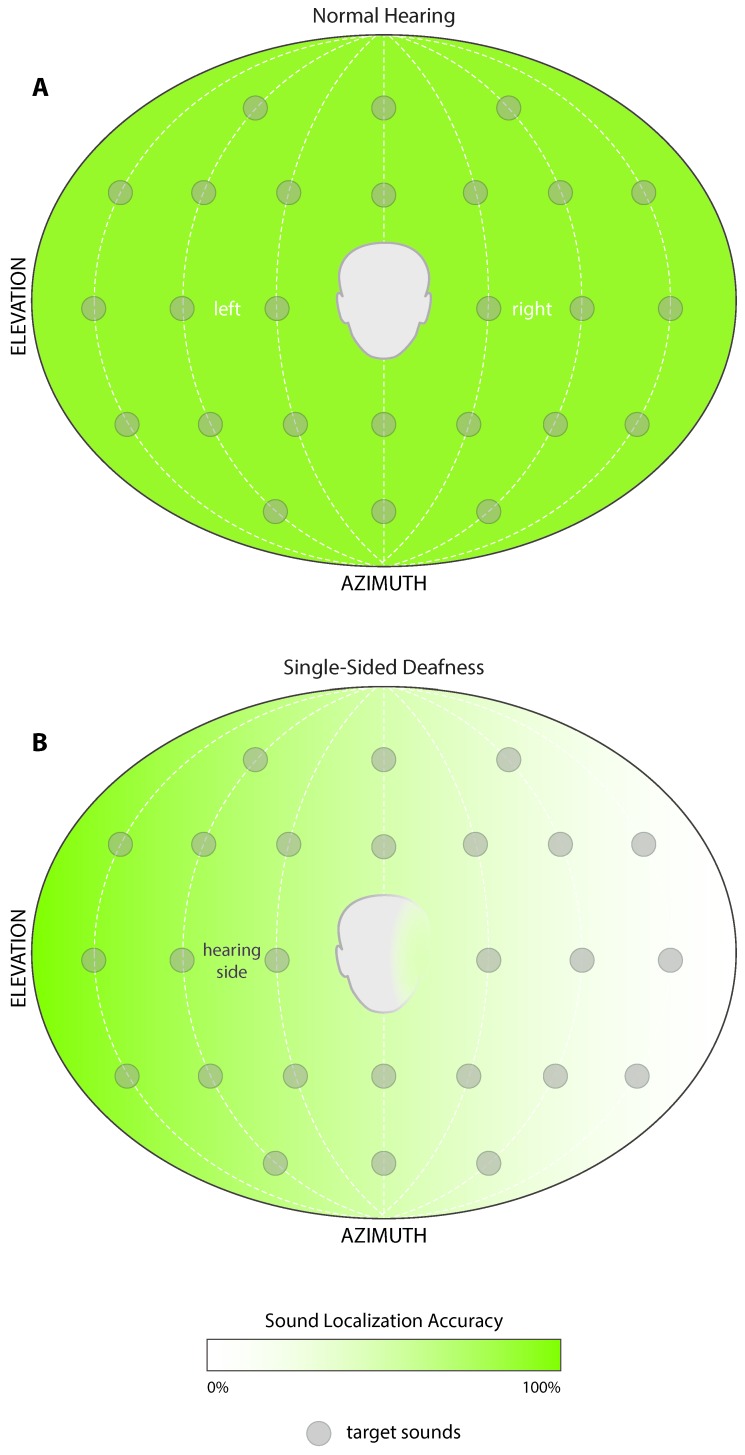
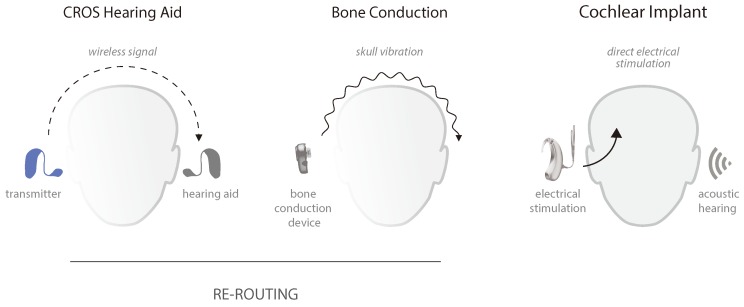
There is an increasing global recognition of the negative impact of hearing loss, and its association to many chronic health conditions. The deficits and disabilities associated with profound unilateral hearing loss, however, continue to be under-recognized and lack public awareness. Profound unilateral hearing loss significantly impairs spatial hearing abilities, which is reliant on the complex interaction of monaural and binaural hearing cues. Unilaterally deafened listeners lose access to critical binaural hearing cues. Consequently, this leads to a reduced ability to understand speech in competing noise and to localize sounds. The functional deficits of profound unilateral hearing loss have a substantial impact on socialization, learning and work productivity. In recognition of this, rehabilitative solutions such as the rerouting of signal and hearing implants are on the rise. This review focuses on the latest insights into the deficits of profound unilateral hearing impairment, and current treatment approaches.
Keywords: cochlear implant; monaural; single-sided deafness; spatial hearing; unilateral hearing loss.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO . Global Estimates on Hearing Loss. World Health Organization; Geneva, Switzerland: 2018. [(accessed on 10 January 2020)]. Available online: http://www.who.int/pbd/deafness/estimates/en/
Publication types
LinkOut - more resources
Full Text Sources
