

Comprehensive routine diagnostic screening to identify predictive mutations, gene amplifications, and microsatellite instability in FFPE tumor material
- PMID: 32264863
- PMCID: PMC7137451
- DOI: 10.1186/s12885-020-06785-6
Comprehensive routine diagnostic screening to identify predictive mutations, gene amplifications, and microsatellite instability in FFPE tumor material
Abstract
Background: Sensitive and reliable molecular diagnostics is needed to guide therapeutic decisions for cancer patients. Although less material becomes available for testing, genetic markers are rapidly expanding. Simultaneous detection of predictive markers, including mutations, gene amplifications and MSI, will save valuable material, time and costs.
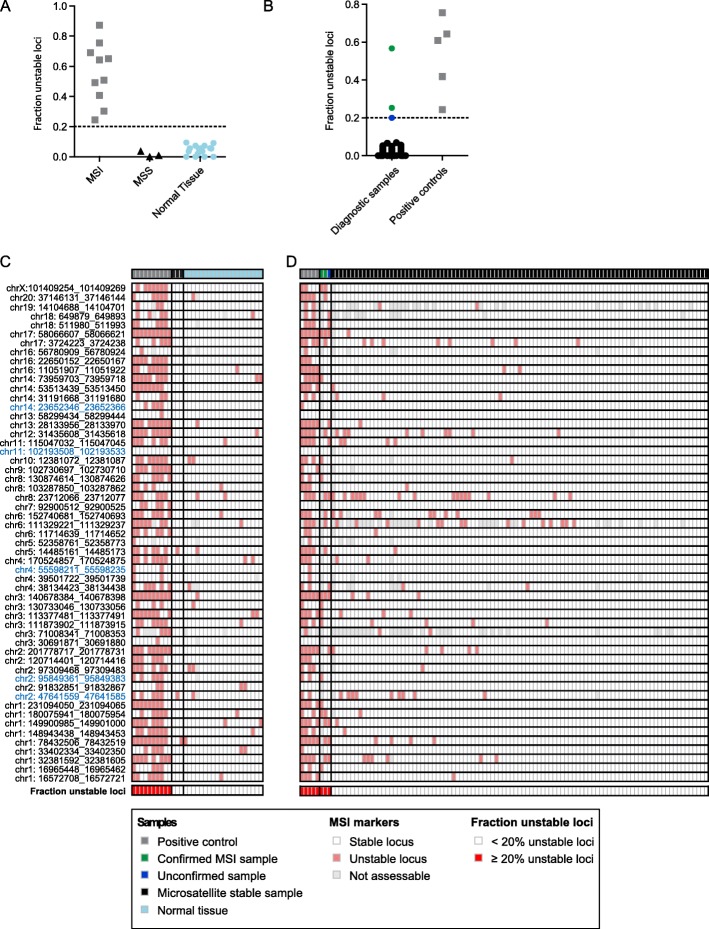
Methods: Using a single-molecule molecular inversion probe (smMIP)-based targeted next-generation sequencing (NGS) approach, we developed an NGS panel allowing detection of predictive mutations in 33 genes, gene amplifications of 13 genes and microsatellite instability (MSI) by the evaluation of 55 microsatellite markers. The panel was designed to target all clinically relevant single and multiple nucleotide mutations in routinely available lung cancer, colorectal cancer, melanoma, and gastro-intestinal stromal tumor samples, but is useful for a broader set of tumor types.
Results: The smMIP-based NGS panel was successfully validated and cut-off values were established for reliable gene amplification analysis (i.e. relative coverage ≥3) and MSI detection (≥30% unstable loci). After validation, 728 routine diagnostic tumor samples including a broad range of tumor types were sequenced with sufficient sensitivity (2.4% drop-out), including samples with low DNA input (< 10 ng; 88% successful), low tumor purity (5-10%; 77% successful), and cytological material (90% successful). 75% of these tumor samples showed ≥1 (likely) pathogenic mutation, including targetable mutations (e.g. EGFR, BRAF, MET, ERBB2, KIT, PDGFRA). Amplifications were observed in 5.5% of the samples, comprising clinically relevant amplifications (e.g. MET, ERBB2, FGFR1). 1.5% of the tumor samples were classified as MSI-high, including both MSI-prone and non-MSI-prone tumors.
Conclusions: We developed a comprehensive workflow for predictive analysis of diagnostic tumor samples. The smMIP-based NGS analysis was shown suitable for limited amounts of histological and cytological material. As smMIP technology allows easy adaptation of panels, this approach can comply with the rapidly expanding molecular markers.
Keywords: Colorectal carcinoma; FFPE; GIST; Gene amplification; Lung cancer; Melanoma; Microsatellite instability; Mutation; Next-generation sequencing; Predictive analysis.
Conflict of interest statement
The authors declare that they have no conflict of interest.
BBJT is a member of the BMC Cancer editorial board, but has not played any role in editorial decisions made regarding this manuscript. Outside the submitted work MJLL has relations with AstraZeneca, Bayer, Bristol-Myers Squibb, Illumina, Janssen pharmaceuticals, Merck, and Nimagen; outside the submitted work LCvK has relations with Janssen pharmaceuticals, Bristol-Myers Squib, Merck, nanoString, and is an advisor for Guidepoint; outside the submitted work ES has relations with AstraZeneca, Roche, Pfizer, Novartis, Bayer, BMS, BioCartis, Illumina, Agena Bioscience, CC Diagnostics, Janssen Cilag (Johnson&Johnson), Diaceutics, Bio-Rad, Abbott, Boehringer Ingelheim, Promega.
Figures



References
-
- Jennings LJ, Arcila ME, Corless C, Kamel-Reid S, Lubin IM, Pfeifer J, Temple-Smolkin RL, Voelkerding KV, Nikiforova MN. Guidelines for validation of next-generation sequencing-based oncology panels a joint consensus recommendation of the Association for Molecular Pathology and College of American pathologists. J Mol Diagn. 2017;19(3):341–365. doi: 10.1016/j.jmoldx.2017.01.011. - DOI - PMC - PubMed
-
- Dietel M, Johrens K, Laffert MV, Hummel M, Blaker H, Pfitzner BM, Lehmann A, Denkert C, Darb-Esfahani S, Lenze D, et al. A 2015 update on predictive molecular pathology and its role in targeted cancer therapy: a review focussing on clinical relevance. Cancer Gene Ther. 2015;22(9):417–430. doi: 10.1038/cgt.2015.39. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
