

Effect of initial infusion rates of fluid resuscitation on outcomes in patients with septic shock: a historical cohort study
- PMID: 32264936
- PMCID: PMC7140334
- DOI: 10.1186/s13054-020-2819-5
Effect of initial infusion rates of fluid resuscitation on outcomes in patients with septic shock: a historical cohort study
Abstract
Background: Fluid resuscitation has become the cornerstone of early septic shock management, but the optimal fluid rate is still not well studied. The goal of this investigation is to examine the relationship between fluid resuscitation rate and septic shock resolution.
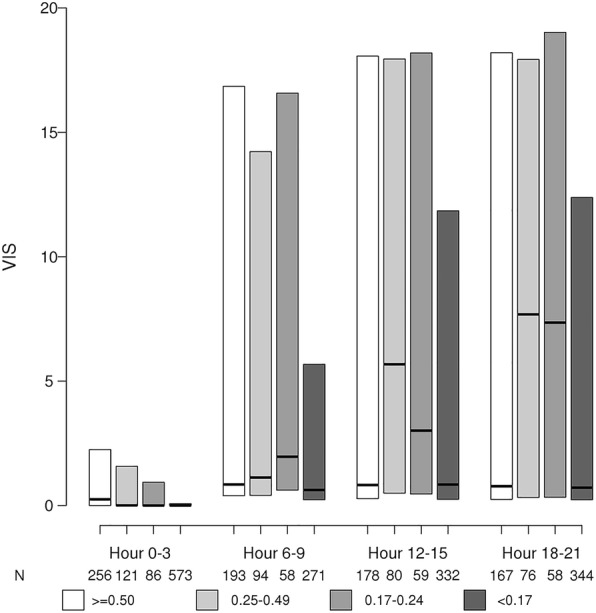
Method: We retrospectively studied adult (≥ 18 years) patients with septic shock, defined based on sepsis III definition, from January 1, 2006, through May 31, 2018, in the medical intensive care unit (MICU) of Mayo Clinic Rochester. The fluid resuscitation time was defined as the time required to infuse the initial fluid bolus of 30 ml/kg, based on the recommendations of the 2016 surviving sepsis campaign. The cohort was divided into four groups based on the average fluid rate (group 1 ≥ 0.5, group 2 0.25-0.49, group 3 0.17-0.24, and group 4 < 0.17 ml/kg/min). The primary outcome was the time to shock reversal. Multivariable regression analyses were conducted to account for potential confounders.
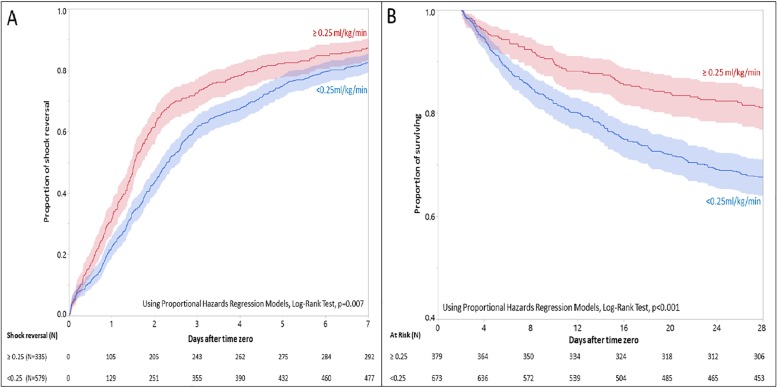
Result: A total of 1052 patients met eligibility criteria and were included in the analysis. The time-to-shock reversal was significantly different among the groups (P < .001). Patients in group 1 who received fluid resuscitation at a faster rate had a shorter time to shock reversal (HR = 0.78; 95% CI 0.66-0.91; P = .01) when compared with group 4 with a median (IQR) time-to-shock reversal of 1.7 (1.5, 2.0) vs. 2.8 (2.6, 3.3) days, respectively. Using 0.25 ml/kg/min as cutoff, the higher fluid infusion rate was associated with a shorter time to shock reversal (HR = 1.22; 95% CI 1.06-1.41; P = .004) and with decreased odds of 28-day mortality (HR = 0.71; 95% CI 0.60-0.85; P < .001).
Conclusion: In septic shock patients, initial fluid resuscitation rate of 0.25-0.50 ml/kg/min (i.e., completion of the initial 30 ml/kg IV fluid resuscitation within the first 2 h), may be associated with early shock reversal and lower 28-day mortality compared with slower rates of infusion.
Keywords: Fluid resuscitation rate; Lactate clearance; Septic shock; Shock reversal; Vasopressor.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
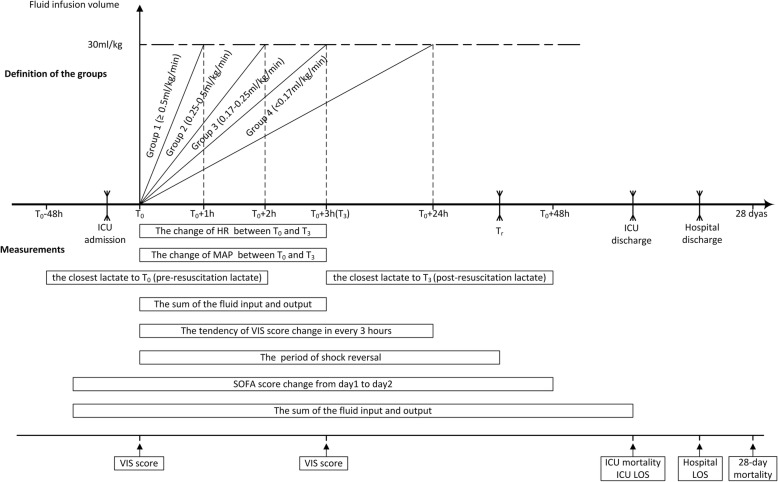
 ” on the timeline marked ICU admission, shock reversal time (Tr), and ICU and hospital discharge; shock reversal time (Tr), ICU discharge, and hospital discharge must be after T0 but had no fixed time relationship with T0. The main variables and measurements of the study are shown in the bottom half of the figure. The period of shock reversal was defined as the duration between Tr and T0 (abbreviation: ICU = intensive care unit; T0 = time zero; T3 = 3 h after T0; Tr = shock reversal time; VIS = Vasoactive-Inotropic Score; LOS = length of stay)
” on the timeline marked ICU admission, shock reversal time (Tr), and ICU and hospital discharge; shock reversal time (Tr), ICU discharge, and hospital discharge must be after T0 but had no fixed time relationship with T0. The main variables and measurements of the study are shown in the bottom half of the figure. The period of shock reversal was defined as the duration between Tr and T0 (abbreviation: ICU = intensive care unit; T0 = time zero; T3 = 3 h after T0; Tr = shock reversal time; VIS = Vasoactive-Inotropic Score; LOS = length of stay)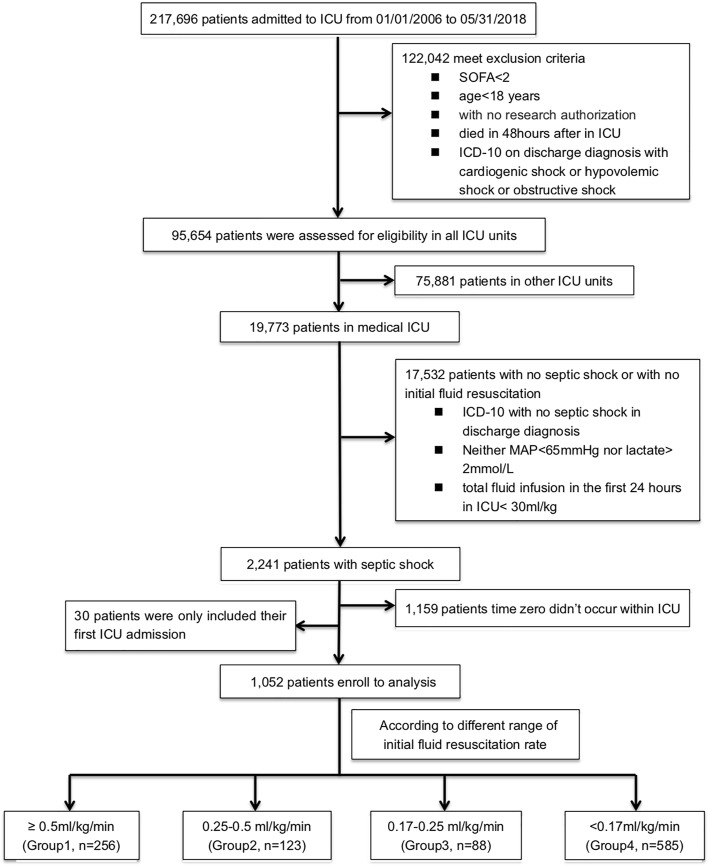
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
