

Abnormal Vital Signs Predict Critical Deterioration in Hospitalized Pediatric Hematology-Oncology and Post-hematopoietic Cell Transplant Patients
- PMID: 32266139
- PMCID: PMC7105633
- DOI: 10.3389/fonc.2020.00354
Abnormal Vital Signs Predict Critical Deterioration in Hospitalized Pediatric Hematology-Oncology and Post-hematopoietic Cell Transplant Patients
Abstract
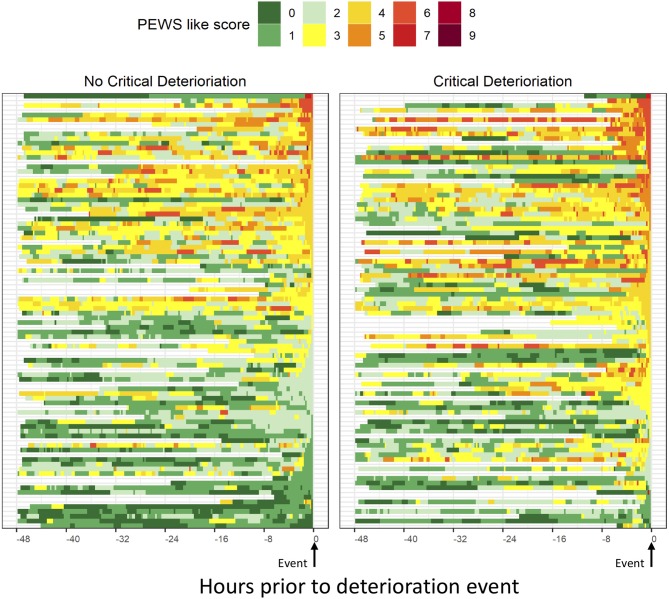
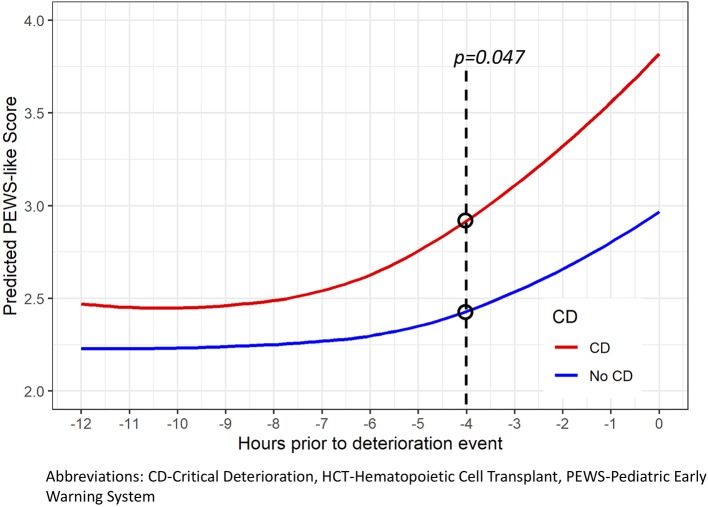
Introduction: Hospitalized pediatric hematology-oncology and post-hematopoietic cell transplant (HCT) patients have frequent deterioration requiring Pediatric Intensive Care Unit (PICU) care. Critical deterioration (CD), defined as unplanned PICU transfer requiring life-sustaining interventions within 12 h, is a pragmatic metric to evaluate emergency response systems (ERS) in pediatrics, however, it has not been investigated in these patients. The goal of this study was to evaluate if CD is an appropriate metric to assess effectiveness of ERS in pediatric hematology-oncology and post-HCT patients and if it is preceded by an actionable period of vital sign changes. Methods: A retrospective review of all unplanned PICU transfers and floor cardiopulmonary arrests in a dedicated pediatric hematology-oncology hospital between August 2014 and July 2016. Vital signs and physical exam findings 48 h prior to events were converted to Pediatric Early Warning System-Like Scores (PEWS-LS) using cardiovascular, respiratory, and neurologic criteria. Results: There were 220 deterioration events, with 107 (48.6%) meeting criteria for CD, representing a rate of 2.98 per 1,000-inpatient-days. Using the first event per hospitalization (n = 184), patients with CD had higher mortality (17.4 vs. 7.6%, p = 0.045), fewer median ICU-free-days (21 vs. 24, p = 0.011), ventilator-free-days (25 vs. 28, p < 0.001), and vasoactive-free-days (27 vs. 28, p < 0.001). Using vital sign data 48 h prior to deterioration events, those with CD had higher PEWS-LS on PICU admission (p < 0.001), spent more time with elevated PEWS-LS prior to PICU transfer (p = 0.008 to 0.023) and had a longer time from first abnormal PEWS-LS (p = 0.007 to 0.043). Significant difference between the two groups was observed as early as 4 h prior to the event (p = 0.047). Conclusion: Hospitalized pediatric hematology-oncology and post-HCT patients have frequent deterioration resulting in a high mortality. In these patients, CD is over 13 times more common than floor cardiopulmonary arrests and associated with higher mortality and fewer event-free days, making it a useful metric in these patients. CD is preceded by a long duration of abnormal vital signs, making it potentially preventable through earlier recognition.
Keywords: Pediatric Early Warning System (PEWS); cardiopulmonary arrest; critical deterioration; emergency response systems; pediatric intensive care; pediatric oncology.
Copyright © 2020 Agulnik, Gossett, Carrillo, Kang and Morrison.
Figures
References
-
- 100K Lives Campaign—Getting Started Kit: Rapid Response Teams. Available online at: http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm (accessed February 7, 2018).
LinkOut - more resources
Full Text Sources