

Secondary Sclerosing Cholangitis in Critically Ill Patients: An Underdiagnosed Entity
- PMID: 32266307
- PMCID: PMC7113589
- DOI: 10.1159/000501405
Secondary Sclerosing Cholangitis in Critically Ill Patients: An Underdiagnosed Entity
Abstract
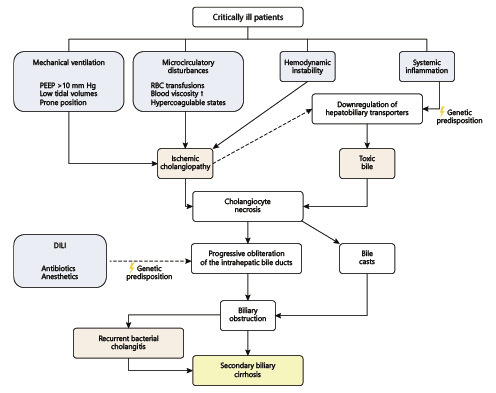
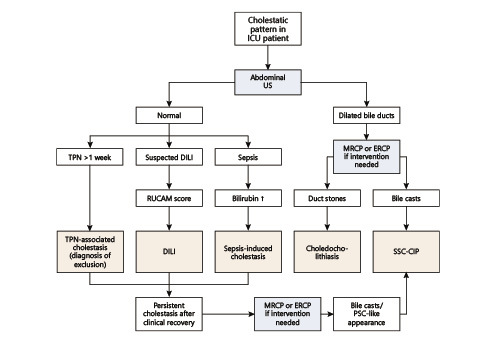
Secondary sclerosing cholangitis in critically ill patients (SSC-CIP) is a recently identified cholestatic liver disease occurring in patients without prior history of hepatobiliary disease, after receiving treatment in the intensive care unit (ICU) in different settings, including cardiothoracic surgery, infection, trauma, and burns. It is a rare entity, being estimated to occur in 1/2,000 patients in an ICU; however, it is a dismal condition, with up to half of the patients dying during the ICU stay and with rapid progression to liver cirrhosis over weeks to months. SSC-CIP should be considered in the differential diagnosis of cholestasis in the ICU, particularly when cholestasis persists after recovery from the critical event. Diagnosis is established with magnetic resonance cholangiopancreatography or endoscopic retrograde cholangiopancreatography showing dilations and stenoses of the intrahepatic bile ducts as well as biliary casts. No available treatment has been shown to slow the rapid progression of the disease, and liver transplant referral should be considered early after the diagnosis of SSC-CIP. Increased awareness and timely diagnosis are crucial in order to improve the current appalling outcome.
A colangite esclerosante secundária em doentes críticos (CEP-DC) é uma doença colestàtica, identificada recentemente, que ocorre em doentes sem antecedentes de patologia hepato-biliar, após internamento em unidade de cuidados intensivos (UCI) por diferentes indicações, incluindo: cirurgia cárdio-torácica, infeção, trauma e queimaduras. É uma entidade rara, com uma incidência estimada de um em cada 2,000 doentes em UCI. Ainda assim, tratase de uma doença com um muito mau prognóstico, sendo que até metade dos doentes morre durante o internamento na UCI, e apresenta uma rápida progressão para cirrose em semanas a meses. A CEP-DC deve ser considerada no diagnóstico diferencial de colestase em UCI, particularmente se a colestase persistir após a recuperação do evento potencialmente fatal. O diagnóstico é estabelecido através de colangiopancreatografia por ressonância magnética ou colangiopancreatografia retrógrada endoscópica, que revelam estenoses e dilatações difusas dos canais biliares intra-hepáticos e cilindros biliares. Não está disponível uma terapêutica capazde atrasar a rápida progressão da doença e a referenciação para transplantação hepática deve ser considerada logo após o diagnóstico. Para melhorar o mau prognóstico atual, é essencial um maior reconhecimento e diagnóstico precoce.
Keywords: Critically ill patients; Intensive care unit; Secondary sclerosing cholangitis.
Copyright © 2019 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Williamson KD, Chapman RW. Primary sclerosing cholangitis: a clinical update. Br Med Bull. 2015 Jun;114((1)):53–64. - PubMed
-
- Brooling J, Leal R. Secondary Sclerosing Cholangitis: a Review of Recent Literature. Curr Gastroenterol Rep. 2017 Sep;19((9)):44. - PubMed
-
- Scheppach W, Druge G, Wittenberg G, Mueller JG, Gassel AM, Gassel HJ, et al. Sclerosing cholangitis and liver cirrhosis after extrabiliary infections: report on three cases. Crit Care Med. 2001 Feb;29((2)):438–41. - PubMed
-
- Leonhardt S, Veltzke-Schlieker W, Adler A, Schott E, Eurich D, Faber W, et al. Secondary Sclerosing Cholangitis in Critically Ill Patients: Clinical Presentation, Cholangiographic Features, Natural History, and Outcome: A Series of 16 Cases. Medicine (Baltimore) 2015 Dec;94((49)):e2188. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
