

Healthcare resource utilization and costs associated with inflammatory bowel disease among patients with chronic inflammatory diseases: a retrospective cohort study
- PMID: 32266326
- PMCID: PMC7114816
- DOI: 10.1186/s41927-020-0115-2
Healthcare resource utilization and costs associated with inflammatory bowel disease among patients with chronic inflammatory diseases: a retrospective cohort study
Abstract
Background: Chronic inflammatory diseases (CIDs; ankylosing spondylitis [AS], psoriatic arthritis [PsA], psoriasis [PsO], or rheumatoid arthritis [RA]) and inflammatory bowel disease (IBD; Crohn's disease and ulcerative colitis) are associated with substantial economic burden. The relative increased costs among patients with CIDs and concomitant IBD compared to those without IBD is an important consideration when deciding on the clinical management of patient symptoms. Given the increasing use of novel agents for the treatment of CIDs, including those that may increase the risk of IBD in patients with CIDs, the objective of the study was to describe the incidence of IBD and to quantify healthcare resource utilization (HRU) and costs associated with IBD among patients with CIDs.
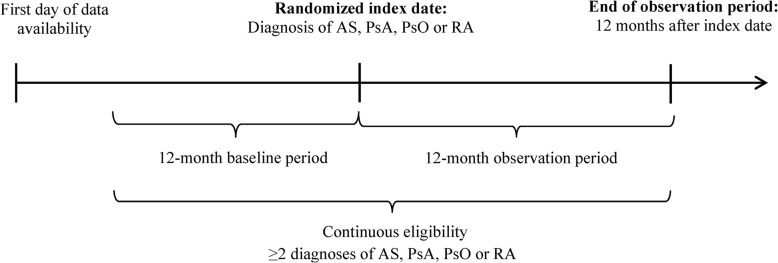
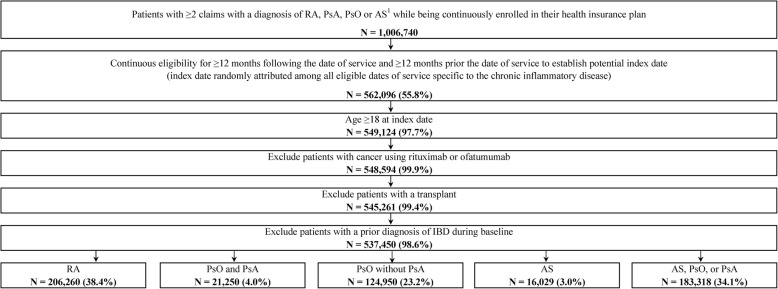
Methods: The IBM MarketScan® Research Databases (1/2010-7/2017) were used to identify adult patients with ≥2 claims with a diagnosis of either AS/PsA/PsO/RA (index date was a random claim for AS/PsA/PsO/RA). The one-year incidence rate of IBD was calculated following the index date. HRU and healthcare costs were compared between patients developing and not developing IBD in the year following the index date, adjusting for baseline characteristics.
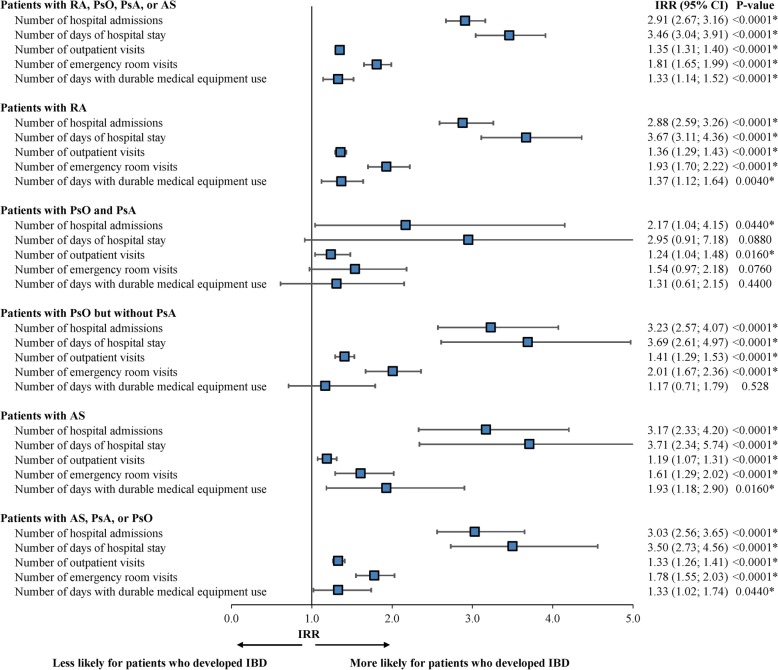
Results: A total of 537,450 patients with CIDs (mean age = 54.0 years; 63.1% female) were included in the study. The 1-year incidence rate of IBD was 0.52% (range = 0.39% in patients with PsO but without PsA to 1.73% in patients with AS). Patients who developed IBD (N = 2778) had significantly higher rates of inpatient, outpatient, and emergency room visits (incidence rate ratios [IRR] = 2.91, 1.35, 1.81; all P < 0.0001), compared to patients without IBD (N = 534,672). Patients who developed IBD had $18,500 (P < 0.0001) higher total costs per year, including $15,121 (P < 0.0001) higher medical costs and $3380 higher pharmacy costs (P < 0.0001).
Conclusion: Higher HRU and costs were observed in patients with concomitant CID and IBD compared to patients with CID alone. Consideration should be given to treatment decisions that adequately manage CID and IBD to ensure optimal clinical and economic outcomes.
Keywords: Ankylosing spondylitis; Crohn’s disease; Healthcare costs; Healthcare resource utilization; Inflammatory bowel disease; Psoriasis; Psoriatic arthritis; Rheumatoid arthritis; Ulcerative colitis.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsBE and PL are employees of Analysis Group, Inc., a consulting company which provided paid consulting services to Janssen Scientific Affairs, LLC for the conduct of this study. SDC, LAE, and KS are employees of Janssen Scientific Affairs, LLC and shareholders of Johnson & Johnson, of which Janssen Scientific Affairs, LLC is a wholly-owned subsidiary. DPH reports the following affiliations: Janssen (consulting), Takeda (consulting), AbbVie (consulting), Salix (consulting), and Pfizer (consulting and research support). JUS reports the following affiliations: Janssen (consulting), UCB (consulting), Novartis (consulting and research support), Amgen (consulting and research support [via NIH Target]), and Pfizer (research support).
Figures


References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
